Hospital: Hospital Universitario Rio Hortega, Hospital Universitario San Cecilio, Hospital Universitario del Sureste de Arganda del Rey.
Nº: C2019-426
Aut@r o Autores: V. Jimenez Coronel, I. Garrido Marquez, L. Diaz Rubia, M. Gutierrez Gallardo.
Presentación
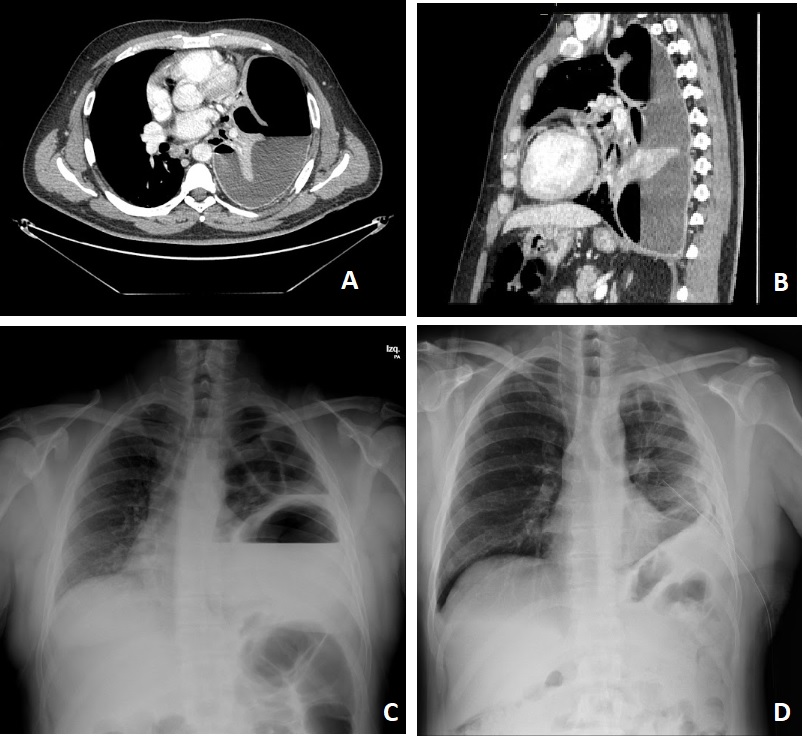
We present the case of a giant lung abscess in an immunocompetent patient. The patient is a 50-year-old male with symptoms of fever and general malaise for several days. The chest X-ray performed in the emergency room reveals a large cavitated lesion with an air-fluid level that occupies almost the entire left lung and causes contralateral mediastinal displacement. Subsequently, a chest CT scan with intravenous contrast was performed to identify the etiology, demonstrating the presence of a large abscess as the cause.
Discusión
Lung abscesses are not infrequent, especially in immunosuppressed or hospitalized patients. They are usually due to aspiration of anaerobic bacteria from the oral flora and are usually polymicrobial. Radiographically, they are visualized as a radiolucent image within a consolidation, nodule or mass with a wall of varying thickness and may have a hydro-aerial level inside it. We must established the differential diagnosis of this entity with empyema, necrotizing pneumonia, infected emphysematous bulla and diaphragmatic hernia due to the size of our case. The majority of lung abscesses do not respond to antibiotic treatment, so we use as an alternative to surgery or transthoracic or endobronchial percutaneous drainage. In our case, due to the size of the abscess, transthoracic percutaneous drainage was required, with a satisfactory evolution of the patient. ?
Conclusión
Lung abscesses are a frequent entity, although they do not usually reach such a large size.It is important to emphasize the role of thoracic CT in these cases to establish the most appropriate diagnosis and establish treatment urgently.13.
Bibliografía
- O.Wali S. An uptodate on the drainage of pyogenic lung abscesses.Ann Thorac Med. 2012 Jan-Mar, 7(1): 3–7. doi: 10.4103/1817-1737.91552 - Walker CM, Abbott GF, Green RE, Shepard JA, Vummidi D, Digumarthy SR. Imaging Pulmonary Infection: Classic Signs an