Hospital: Hospital Universitario Morales Meseguer, Hospital Morales Meseguer.
Nº: C2019-421
Aut@r o Autores: M. Lozano Ros, A. Blanco Barrio, E. Girela Baena, I. Vicente Zapata, I. González Moreno, G. Pérez Hernández.
Presentación
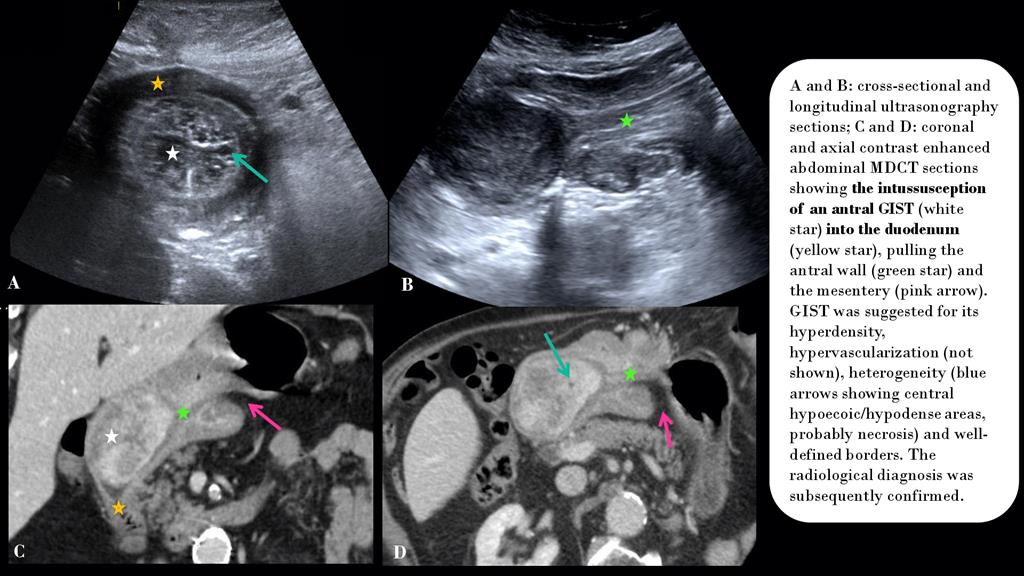
An 83-year-old man presented to the Emergency Department (ED) complaining of epigastric pain and vomiting for the last few hours, without diarrhea, fever or other symptoms. He had come to the ED with similar episodes in the previous months. Previous cholecystectomy. Ultrasonography and subsequent abdominal MDCT were performed, showing a heterogeneous, well-defined, vascularized, submucosal antral mass acting as the lead point of an antro-duodenal intussusception. The mass was 7 x 6 x 5 cm and its radiological features were consistent with a GIST tumor. The surgical findings were consistent with the radiological findings and the pathological study confirmed a GIST tumor type. Partial gastrectomy and Y-en-Roux reconstruction were performed.
Discusión
Intussusception consists of the telescoping of a bowel segment into the lumen of the contiguous part of the intestinal tract. It is a rare cause of bowel obstruction in adults (< 5%), being mostly caused by structural lesions. Gastric intussusception is an even more rarely documented condition. Clinical presentation is nonspecific making diagnosis challenging. Diagnosis is best made by CT in adults, although US is also very useful. Intussusception appears as a complex mass consisting of the outer intussuscipiens and the central intussusceptum, with the lead point distal to the tapered lumen of the intussusceptum. CT will show a pathognomonic bowel-within-bowel configuration with or without contained mesenteric fat/vessels. Intussusception appears as a sausageshaped mass when the CT section is parallel to its longitudinal axis and as a target-like mass when the section is perpendicular to the longitudinal axis. Ultrasound will show the characteristic target-like or bull's eye sign, similar to the CT findings. In our case, the antral tumor acted as the lead point. There were foreshortening and narrowing of the gastric antrum and widening of the duodenum. The location and radiological features (heterogeneity, well-definition, hypervascularization) of the mass were consistent with a GIST tumor. These tumors rarely intussuscept as they are usually exophytic. When identified, we should look for metastases. Management of intussusception depends on the underlying lesion. Benign etiologies causing transient non-obstructing intussusception can be managed conservatively (celiacsprue, Crohn’s disease). Surgery is necessary in cases of malignancy, obstruction and ischemia.
Conclusión
Intussusceptions are a rare cause of bowel obstruction in adults. We should look for structural lesions in order to guide the appropriate treatment.
Bibliografía
- Hong Choi S, Koo Han J, Hyung Kim S, Min Lee J, Ho Lee K, Jun Kim Y et al. Intussusception in Adults: From Stomach to Rectum. AJR Am J Roentgenol, 2004,183(3):691-8. - Rabbani K, Narjis Y, Finech B and Elidrissi A. Unusual malignant cause of adult intu