Hospital: Hospital Universitario Joan XXIII Tarragona.
Nº: C2019-720
Aut@r o Autores: M.V. Orellana Vélez, A. Samitier, O. Mezosi, S. Ricart, A. Chacón.
Presentación
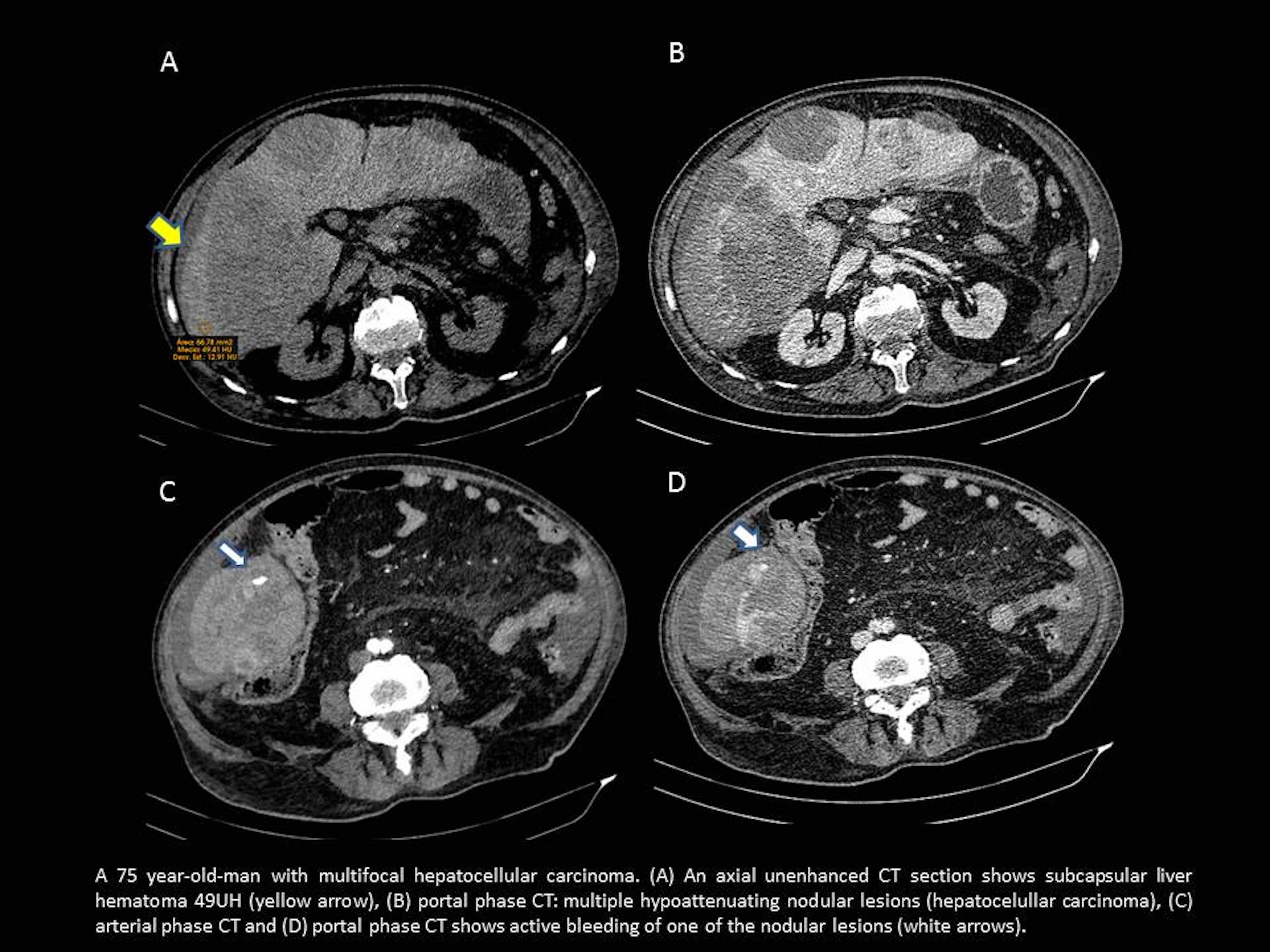
A 75 year old man presented at the emergency department of our hospital with sudden onset of malaise accompanied by abdominal pain in the right upper quadrant, generalized weakness and vegetative pain with sweating and nausea. It does not present depositional alterations. He had a history of multifocal hepatocellular carcinoma plus right portal thrombosis of recent diagnosis in a computed tomography (CT) two months ago. During physical examination, his blood pressure was 90/70 mmHg, and his pulse rate was 80beats/min. The results of a peripheral blood examination were the following: white blood cells 14220/mm3, platelet count 440000/mm3, hemoglobin 7.8g/dL, hematocrit 25.2%, and C-reactive protein 3.2 mg/dL. Helical abdominal acquisition is performed before, during and after the administration of intravenous contrast. Comparative evaluation with respect to previous study 2 months ago was: hemoperitoneum, increase in liver size at the expense of multiple nodular lesions. Within a liver lesion in the lower pole (theoretical s.VI), we observe a focus of contrast extravasation in arterial phase and accumulation in delayed phase that suggests active bleeding. It is appreciated subcapsular liver hematoma too.
Discusión
Hepatocelullar carcinoma (HCC) is the most common primary liver malignancy. Spontaneous hemorrhage of HCC is a serious complication with high mortality. The incidence of spontaneous rupture in HCC has been reported as being between 3% and 26%. The incidence of spontaneous hemorrhage in HCC is higher in Asia and Africa than in Europe. The mechanism remains unclear, but it could by fluctuation in systolic blood pressure, large central tumours that destroy arteries o veins, traumatic laceration, pressure from tumour growth, central necrosis, presence of coagulopathy or a mixture of all. Diagnosis may be made with clinical examination but CT findings are really helpful. The symptoms of this case (abdominal pain, hemodynamic instability, peritoneal irritation and shock) are the most common clinical presentation and it means that frequently is associated with primary hepatic tumors, such as hepatocellular carcinoma or hepatic adenoma, which have greater vascularity than metastatic lesions. Shock has been presented in 33-90% of the cases. It is true that if we know this patient's background (hepatocellular carcinoma), it is easier to associate the carcinoma with active bleeding, but it is still rare.
Conclusión
Spontaneous hemorrhage in HCC should be considered as a primary differential diagnosis in spontaneous hemoperitoneum in patients with a liver lesion or lesions. We have to act quickly because it is a pathology that causes haemorrhagic shock and death. The use of correct CT protocol imaging facilitated the prompt diagnosis and subsequent treatment.
Bibliografía
- Özen O, Tosun A, Akgül C. Spontaneous rupture of multifocal hepatocellular carcinoma: case report. Internacional Medical Case Reports Journal 2015, 8:165-167. - Pinal DF, Nuño CM, Gómez A, Corona JL, Espejo I. Spontaneous rupture of hepato