Hospital: Hospital Universitario Morales Meseguer, HOSPITAL MORALES MESEGUER.
Nº: C2019-564
Aut@r o Autores: J. Trejo Falcón, A. Moreno Pastor, A. Blanco Barrio, M. López Poveda, I. González Moreno, I. Herves Escobedo.
Presentación
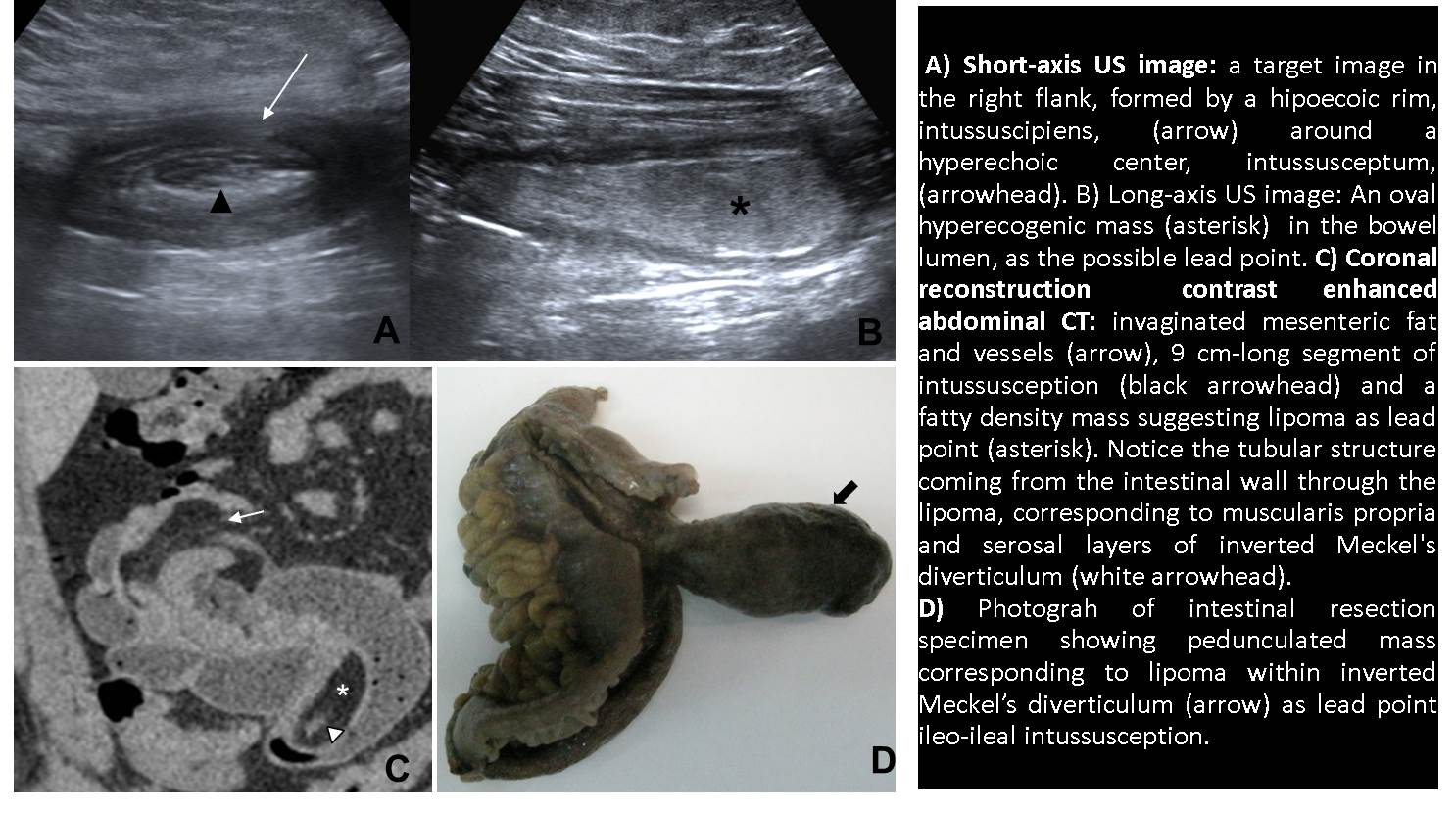
A 36-year-old male presented to the Emergency Department with right iliac fossa pain, leukocytosis and positive Blumberg on physical examination. Findings description: Ultrasound imaging revealed a target sign on the right flank, characteristic of intussusception, formed by a hypoechoic ring from the edematous walls of the intussuscipiens around a hyperechoic center of the intussusceptum. Also was identified an oval hyperechoic image as the pathologic lead point. Under suspicion of intussusception, a contrast enhanced abdominal CT was performed that showed in the distal ileum lumen, a polypoid 5 cm x 2 cm fatty density mass with enhanced thin wall, suggesting submucosal lipoma as the leading point of a 9 cm-long segment of intussusception. Proximal to the lipoma there is feculent appearing material within the small bowel, in keeping with a degree of obstruction. Laparotomy confirmed a benign submucosal tumor concordant with lipoma, as underlying cause of ileo-ileal intussusception, 16 cm from the ileocecal valve. Pathologic evaluation identified within the submucosal lipoma a nest including some glandular structures without significant atypia, surrounded by all intestinal wall layers, suggesting Meckel’s diverticulum. Retrospectively, on the CT scan we could identify a pedunculated structure at the base of the lipoma correspondent to muscularis propria and serosa layers of inverted Meckel’s diverticulum.
Discusión
Small bowel intussusception is usually transient without a lead point. When it occurs, a lead point is normally a benign mass, such as lipoma or inverted Meckel diverticulum. Lipomas originate in the submucosal layer and mostly appear as a sessile protrusion into the bowel lumen. Due to motor activity of underlying muscularis propria, lipomas tend to extrude through the luminal area progressively, which might be the responsible reason for the inversion of the Meckel’s diverticulum in our case. In this manner, a pseudopedicle is formed, providing a polypoid appearance to the lesion. The location of the fat component within the Meckel's diverticulum was in the submucosal layer. This finding is important to differentiate a lipoma from a pseudolipoma in an inverted Meckel's diverticulum, where invaginated mesenteric fat can be misdiagnosed as a lipoma.
Conclusión
Tumors within a Meckel’s diverticulum occur infrequently. Moreover, intussusception caused by a lipoma within the Meckel’s diverticulum is so uncommon with a very few cases reported in the literature.
Bibliografía
- Güldeniz K. et al. Lipoma within inverted Meckel’s diverticulum as a cause of Recurrent partial intestinal obstruction and hemorrhage: A case report and review of literature. World J Gastroenterol 2007 February 21, 13(7): 1141-1143. - Kim KH et al. In