Hospital: Hospital Morales Meseguer, Hospital Santa Lucía.
Nº: C2019-559
Aut@r o Autores: B. Márquez Argente Del Castillo, A. Moreno Pastor, M. Lozano Ros, I. González Moreno, C. Botía González, I. Cases Susarte.
Presentación
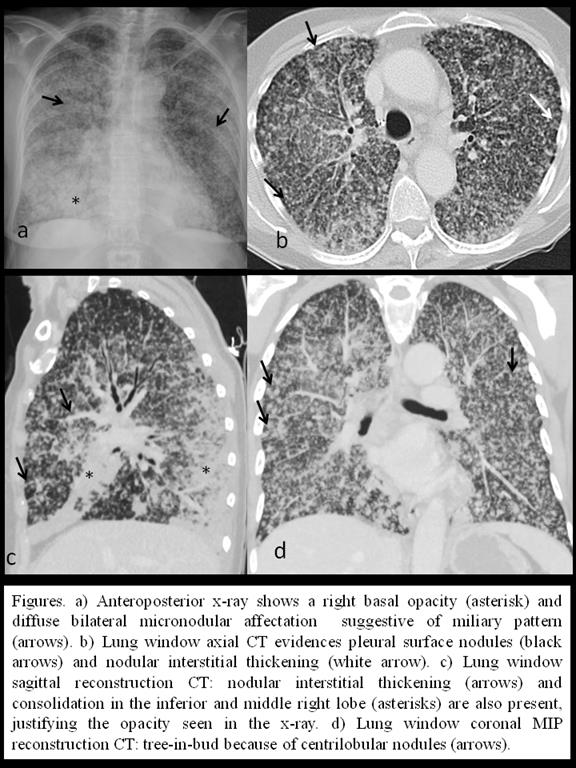
A 66 year old female presented to the emergency department with pulmonary infection symptoms and constitutional syndrome. As relevant findings in medical history the patient had a melanocytic familiar syndrome and a melanoma excision thirty years ago. Imaging findings: An anteroposterior chest x-ray performed at the emergency department (figure a) showed a diffuse lung affectation by miliary nodules and a right basal opacity. To determine the miliary pattern etiology, a contrast enhanced chest and abdominal CT was performed (figures b, c and d). Lung window CT images demonstrated a bilateral and diffuse affectation of the lung parenchyma by random micronodules confirming the miliary pattern. Overlapped, lower lobes ground glass opacities, consolidations, centrilobular nodules and tree-in-bud were seen, suggesting airway affectation. Pleural surface nodules were also detected, implying lymphatic affectation. Two days later, brain-CT evidenced lesions compatible with metastases. The transbronchial biopsy confirmed the diagnosis of a well-defined non mucinous lepidic adenocarcinoma (LA), known before as “non-mucinous bronchioloalveolar carcinoma”.
Discusión
The CT findings showed random, centrilobular and perilymphatic nodules, indicating hematologic, air-way and lymphatic affectation respectively [1, 2]. The differential diagnosis of miliary pattern (random nodules) is usually classified depending on the fever presence (tuberculosis, fungal, viral or rare bacterial infections) or absence (hystocitosis, sarcoidosis, environmental diseases, fungal infections, metastases or miliary tuberculosis) [1, 2]. Because of the melanoma history, both infectious and metastases were considered. Not only centrilobular (accompanied by tree-in-bud) but also non-clustered or random pleural surface nodules can be in relation with an infection. Nevertheless, random nodules also could mean malignant entities [3]. Accordingly, the findings are compatible with both metastases (melanoma history) and infection (mainly tuberculosis). In spite of the melanocytic syndrome and melanoma history, the anatomopathologic diagnosis confirmed a lepidic adenocarcinoma, which typical features at CT agree with our case. LA is distinguished by its growth along alveolar septa and its tendency forbronchial and lymphatic spread. The common presentation of LA is diffuse or multifocal consolidation areas with air-bronchograms or cystic spaces. Instead, random and centrilobular multiple small and defined nodules can appear and mimic haematogenous metastases [3].
Conclusión
Miliary pattern nodules have a wide differential diagnosis but clinical history could lead as to the most probably options. Besides imaging findings suggest infection, tumoral causes should not be forgotten, keeping in mind options like lepidic adenocarcinoma.
Bibliografía
- Webb WR, Müller NL, Naidich DP. High-Resolution CT of the lung. 3rd ed. Philadeplphia: Lippincott Williams & Wilkins, 2001. - Raoof S, Amchentsev A, Vlahos L, Goud A, Naidich DP. Multinodular Disease: A High-Resolution CT Scan Diagnostic Algorithm. Ches