Hospital: Complejo hospitalario universitario de Albacete,
Nº: C2019-34
Aut@r o Autores: Á. Fernández López, S. Atiénzar Jiménez, R. Rodenas Lozano, M.J. Pedrosa Jiménez, J.D. Molina Nuevo, D. Caldevilla.
Presentación
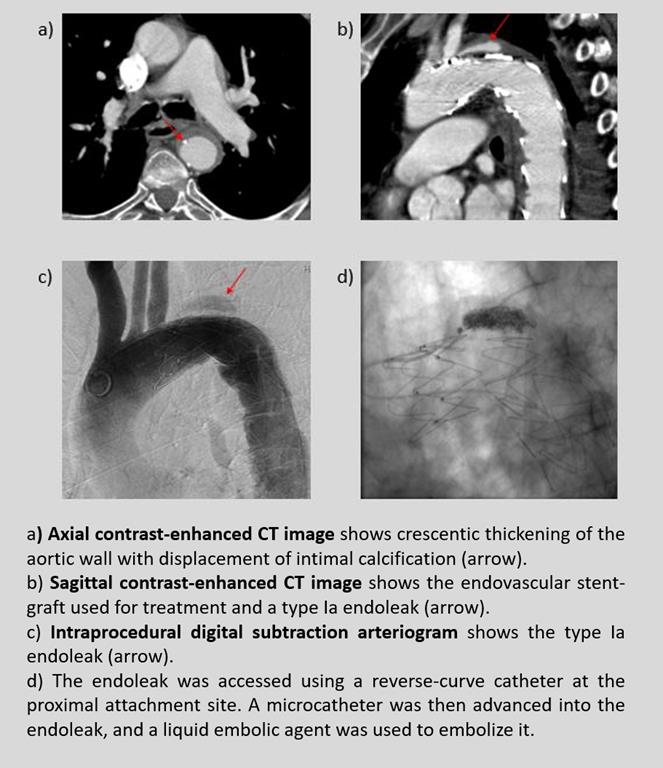
An 81-year-old male with a history of hypertension, smoking habit and chronic obstructive pulmonary disease presented to the emergency department with acute onset of severe back pain. He had been followed in our institution's cardiology department for the last months for chronic chest pain. The vital signs were within normal ranges. A computed tomographic angiogram (CTA) demonstrated an aortic intramural hematoma Stanford type B (without aortic arch involvement). The patient underwent endovascular aortic repair with a stent-graft. Although intraprocedural angiography did not show any endoleaks and the patient was asymptomatic after intervention, a follow-up CTA a week later showed an accumulation of contrast agent within the intramural hematoma outside the graft on arterial phase imaging, around its proximal attachment site, suggestive of an active type Ia endoleak. The patient underwent an aortogram and endovascular embolization of the endoleaks using a liquid embolic agent with an excellent result.
Discusión
Intramural hematoma is included in the spectrum of acute aortic syndrome and appears as an area of hyperattenuating crescentic thickening in the aortic wall that is best seen at nonenhanced computed tomography. It is believed to originate from ruptured vasa vasorum in the aortic media. An endoleak presents as blood flow outside an endograft. It has been documented as the most common complication following endovascular aortic repair. There are five types, which are classified according to the source of blood flow into the endoleak. The type of endoleak will determine the patient´s treatment and follow-up protocol. Type II endoleaks are the most common and result from collateral retrograde flow from the aortic branches. Many of them spontaneously resolve so they are considered benign. Type 1(a or b) endoleak is a persistent perigraft channel of blood flow that is caused by an inadequate seal at either the proximal (a) or the distal (b) end of the stent-graft. This type of endoleak is associated with pressurization of the “aneurysm sac” with systemic pressure, progressive growth risk, and ruptura risk, therefore, it should always be treated. Embolization techniques play an important role in the treatment of endoleaks.
Conclusión
Intramural hematoma is included in the spectrum of acute aortic syndrome and the endovascular repair is the preferred treatment for many people. The most common complications are endoleaks. There are five types, which will determine the patient´s treatment and follow-up protocol. A type I endoleak occurs when there is a gap between the graft and the vessel wall at “seal zones” and it should always be treated.
Bibliografía
- Gutschow S, Walker C, Martínez-Jiménez S, Rosado-de-Christenson M, Stowell J, Kunin J. Emerging Concepts in Intramural Hematoma Imaging. RadioGraphics. 2016,36(3):660-674. - Bryce Y, Rogoff P, Romanelli D, Reichle R. Endovascular Repair o