Hospital: Hospital Ramón y Cajal.
Nº: C2019-609
Aut@r o Autores: R. Romera Sánchez, C. Picón Serrano, I. García Gómez Muriel, A. Olavarria Delagado, A. Palomera Rico, C. Campos Ferrer.
Presentación
29-year-old female with a personal history of left inferior lobectomy for bronchiectasis and ovarian cysts. She has abdominal pain in hypogastrium, colic type, not irradiated, which worsens with movements. Physical examination she is tachycardic and without fever. Analytical values show an elevation of PCR and leukocytosis with neutrophilia. In ultrasound performed by gynecology service only describe suggestive image with teratoma of 12 cm without being able to determine laterality. Due to poor pain control and absence of bowel movements in the last two days, we were asked for complementary imaging test.
Discusión
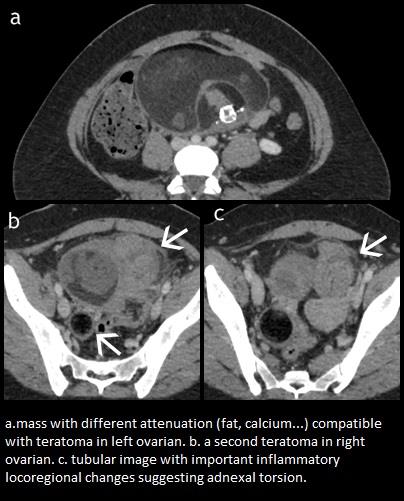
We performed an abdominal CT with intravenous contrast that demonstrated the existence of two lesions, with heterogeneous density composed of fat, areas with intermediate density and in the largest, 15 centimeters, calcium compatible with teratomas. The small size with clear right dependence, the largest, was in the middle line, even right parasagittal, but it was possible to follow the left gonadal vessels until the lesion. Adjacent to the larger teratoma, we found a clearly extraperitoneal tublar structure, which showed thickened walls, accompanied by vascular ingurgitation, discrete ascites and fat stranding. Ovarian teratomas represents the 20% of adult ovarian tumors. Are a group of different histological types composed of the three layers of germinal cells, ectoderm, mesoderm, and endoderm. At CT, fat attenuation within a cyst, with or without calcification in the wall, is diagnostic for mature cystic teratoma. Ovarian teratomas are associated with several complications: torsion, rupture, malignant transformation, infection, andautoimmune hemolytic anemia. The most frequent complication is torsion, which can affect only the ovary, the tube or both, affecting the vascular pedicle. Clinically they present as sudden pain in the lower quadrant, which may or may not be accompanied by nausea and vomiting. CT finding included fallopian tube thickening, smooth wall thickening of the twisted adnexal cystic mass, ascites, and uterine deviation to the twisted side.
Conclusión
It is very important to know the different complications of teratomas and their different clinical manifestations in order to make early diagnosis to preserve the affected ovary and prevent misdiagnosis.
Bibliografía
- Rha SE, Byun JE, Jung SE, Jung JI, Choi BG, Kim BS, et al. CT and MR Imaging Features of Adnexal Torsion. RadioGraphics 2002, 22:283–294. - Iraha Y, Okada M, Iraha R, Azama K, Yamashiro T, Tsubakimoto M, et al. CT and MR Imaging of Gynecologic Emerge