Hospital: Hospital de 12 Octubre.
Nº: C2019-644
Aut@r o Autores: Z. Chen Zhou, J.Z. Ramírez Calderón, L. Ibáñez, R. Sanz De Lucas, L. Hernández Martínez, I. Ríos Gómez.
Presentación
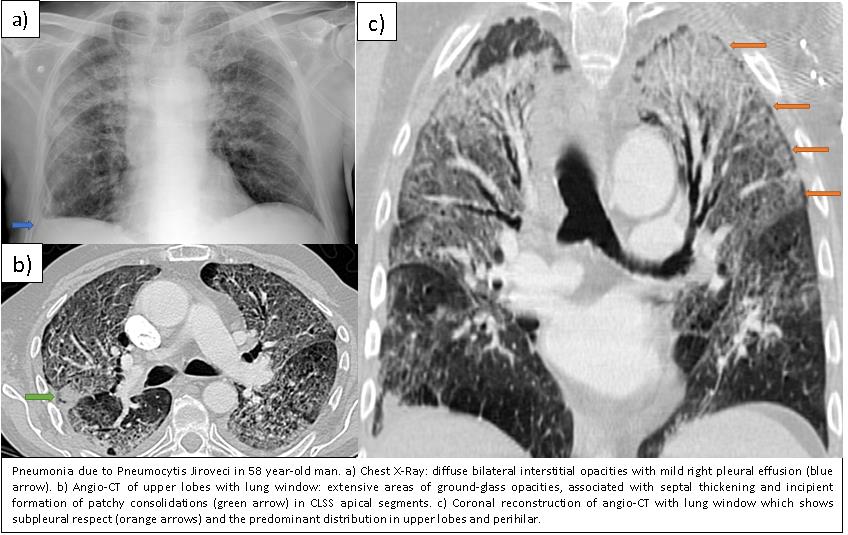
A 58-year-old man, with a history of lung cancer who underwent surgery in February 2018 and was under treatment with corticosteroids and radiotherapy, went to the emergency department for dyspnea, fever and greenish expectoration. The chest X-ray showed diffuse bilateral interstitial opacities. Antibiotic treatment was given, however, during his stay he presented hemoptysis with desaturation and anemia. The Angio-CT of pulmonary arteries showed extensive areas of ground-glass opacities, predominantly in upper lung fields and perihilar, with some subpleural respect, associated with septal thickening and incipient formation of patchy consolidations in CLSS apical segments, suggestive of infectious pathology (first possibility Pneumocystis jiroveci). -
Discusión
Pneumocystis Jiroveci (PJ) is an atypical fungus, opportunistic extracellular pathogen that parasitizes the respiratory tree of the humans. The infection mainly occurs in immunosuppressed patients, especially in cell-mediated immunodeficiencies, as patients with AIDS, oncological history with chemotherapy or radiotherapy, long-term corticoid treatment ... The clinical presentation can be very nonspecific, fever, dry cough, dyspnea, anorexia or weight loss. It must also be kept in mind that in immunosuppressed patients without HIV a much more severe inflammatory response occurs, which in many cases is much more rapid, so these patients can need admission to the ICU. One third of infected patients have normal radiography. The findings are usually nonspecific: bilateral and symmetrical diffuse opacities, preferably perihilar. The main findings of PJ infection in HRCT are an extensive ground-glass opacities with a central distribution and a relative preservation of the periphery. A predilection for the upper portions of the pulmonary lobes has been described. In more advanced stages of the disease, consolidations and thickened septal lines superimposed on the ground-glass opacities can be developed (“crazy paving” pattern). Pulmonary cysts or pneumatoceles occur in up to one third of patients with PJ infection and have been associated with treatment with inhaled pentamidine. Patients recovering from PJ pneumonia may present a complete recovery with total radiological resolution or residual interstitial fibrosis.
Conclusión
PJ pneumonia should be suspected in immunosuppressed patients with symptoms of pulmonary and / or systemic disease, accompanied by ground glass opacities. High-resolution CT has to be performed for evaluation of immunosuppressed patients with suspected pneumonia and normal chest radiographic findings.-
Bibliografía
- Kanne JP, Yandow RD, Meyer CA. Pneumocystis jiroveci Pneumonia: High-Resolution CT Findings in Patients With and Without HIV Infection. AJR. 2012,198: 555–561. - Vogel MN, Brodoefel H, et al. Differences and similarities of cytomegalovirus and pneumocy