Hospital: Hospital Universitario Ramón y Cajal.
Nº: C2019-235
Aut@r o Autores: J. Quintana Pérez, A. Arribas Marcos, R. García Latorre, P. Marazuela García, E. García Santana, A. Vicente Bártulos.
Presentación
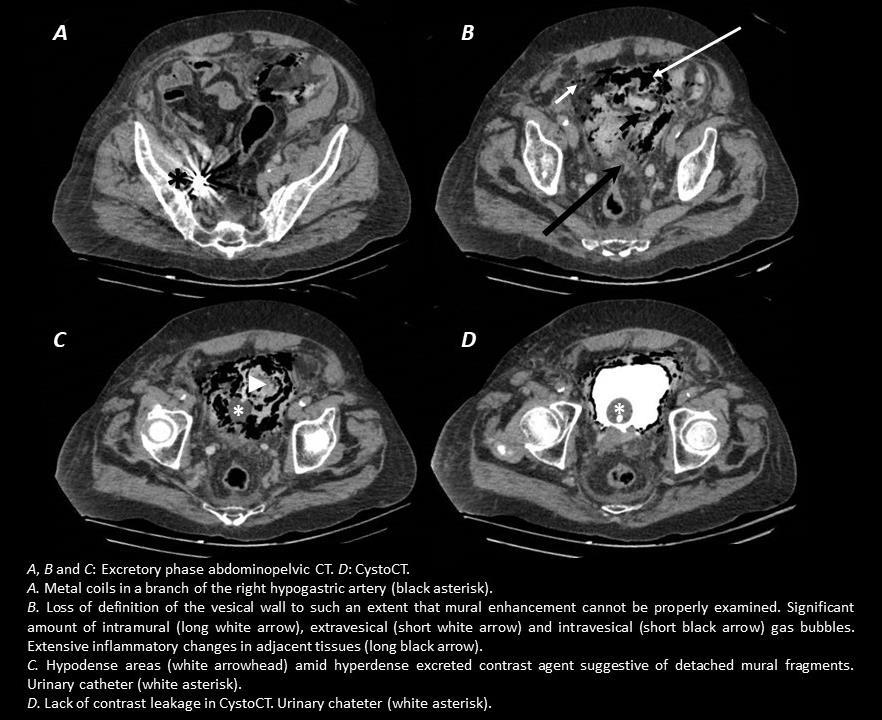
2 year-old male with a history of multifactorial recurring vesical haematuria underwent selective embolization of vesical arteries and vesical floor branches originating from the right hypogastric artery after having exhausted all other therapeutic strategies. In the second day post-embolization the patient started complaining with intense low abdominal pain and signs of peritoneal irritation, there was no evidence of infection. An emergent abdominopelvic CT was performed. Venous and excretory phase series were acquired. A loss of definition and discontinuation of the vesical wall, a remarkable amount of probably intramural, intravesical and extravesical gas bubbles and inflammatory changes in the neighbouring tissues were noted. Hypodense intravesical areas consistent with free detached mural fragments amid hyperdense excreted contrast medium were present in the vesical lumen. The study was completed with intravesical contrast medium administration (cystoCT), which yielded no evidence of contrast leakage.
Discusión
The aforementioned radiological findings were consistent with ischaemic vesical necrosis. Selective vesical arterial embolization with or without hypogastric arterial branch embolization aims at resolving incoercible or recurring haematuria. Materials such as polyvinyl alcohol nanoparticles are used in order to occlude medium calibre vessels, in such a way that an optimal balance between ischaemic risk and recurrence risk is achieved. Vesical necrosis is an uncommon complication of this technique, risk is higher when hypogastric branches are also embolised. Suggestive CT findings include: - Loss of definition and discontinuation of the vesical wall - Wall enhancement alterations - Free detached mural fragments and debris on the inside of the bladder - Intramural gas bubbles, which can spread towards neighbouring areas and might be seen inside and outside the bladder. Lack of infection signs and presence of potential triggers for vesical ischaemia are crucial to distinguishing ischaemic vesical necrosis from emphysematous cystitis as the cause for intramural gas - Inflammatory changes in the adjacent tissuesCystoCT might be useful to demonstrate contrast leakage consistent with perforation.
Conclusión
Vesical necrosis is an urgent infrequent complication of vesical arterial embolization, especially if hypogastric artery branches are also occluded. CT findings include loss of definition of the vesical wall, wall enhancement alteration, intravesical detached mural fragments and intramural gas. CystoCT might be useful to demonstrate perforation.
Bibliografía
- Argüelles Salido E, Medina López RA, Iglesias López A, Congregado Ruiz CB, Peiró de las Heras J, Pascual del Pobil Moreno JL. Embolización arterial selectiva en el tratamiento de la hematuria incoercible. Arch Esp Urol, 2005,