Hospital: HOSPITAL UNIVERSITARIO DE 12 OCTUBRE.
Nº: C2019-624
Aut@r o Autores: E. Martinez-Chamorro, L. Ibañez, G. Garcia-Galarraga, M. Depetris, I. FernandezMarin, S. Borruel.
Presentación
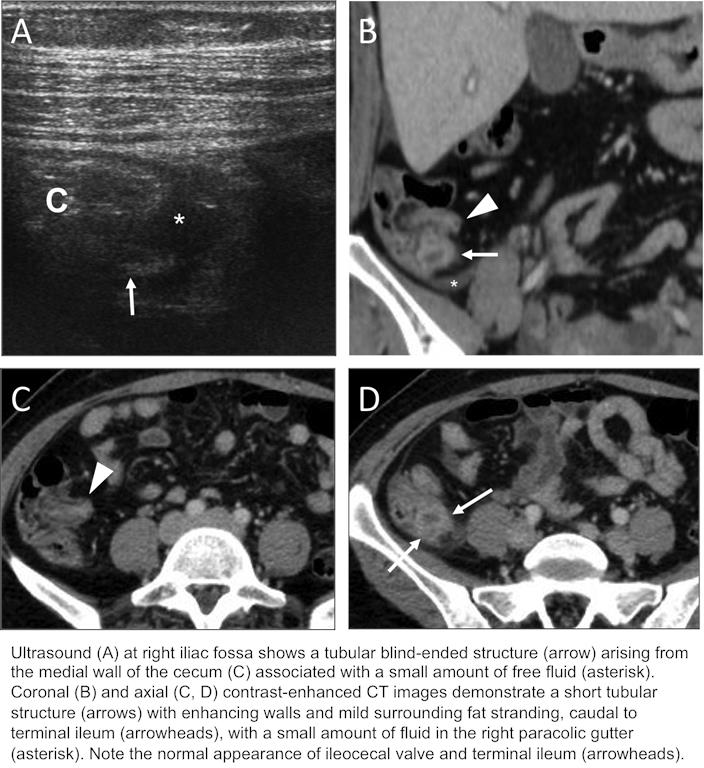
A 45-year-old woman presented to the Emergency Room for a 5-day history of right lower quadrant pain of increasing intensity, associated with fever up to 38.3ºC. Her past medical history was significant for an open appendectomy 4 years ago. Abdominal examination showed a well-healed McBurney’s scar and tenderness in the right lower quadrant. Routine laboratory tests were remarkable for a white cell count of 13.200 cells/mm3 with 93% neutrophils and C-reactive protein of 7.33 mg/dL. Abdominal sonography and contrast-enhanced CT showed a small blind-ended tubular structure extending from the cecum, just below the ileocecal valve, consistent with a dilated appendiceal stump with inflammatory changes in the adjacent fat and a small amount of free fluid. She was managed conservatively with intravenous antibiotics and was discharged 7 days later without complications.
Discusión
Stump appendicitis is a very rare complication of appendectomy, with a reported incidence of 1:50,000 cases of appendectomy. It refers to the inflammation of residual appendiceal tissue after incomplete appendectomy. It has been described in open and laparoscopic appendectomies and the onset interval from initial appendectomy ranges from 2 weeks to 50 years. The clinical presentation does not differ from acute appendicitis, but its diagnosis and treatment are often delayed by the previous history of appendectomy, which may cause the progression of the disease with gangrene, perforation, phlegmon, abscess, and diffuse peritonitis, increasing morbidity and mortality. Diagnostic imaging criteria are the same as those of acute appendicitis. In order to identify the appendix or a possible appendiceal stump, it is important to point out that the relationship between the base of the appendix and the cecum is essentially constant, approximately 3 cm below the ileocecal valve, although the remainder of the appendix is free and the position of the cecum is also variable. MDCT is more helpful in perforated appendicitis. Signs of perforated appendicitis include phlegmon, abscess, extraluminal gas, extraluminal appendicolith, and focal defect in the enhancement of the appendiceal wall.Treatment is usually surgical, but conservative treatment has also been used successfully as in our case.
Conclusión
Stump appendicitis should be considered in the differential diagnosis for patients with previous appendectomy who present with signs and symptoms similar to appendicitis. Imaging tests, ultrasound and CT, play a key role in diagnosis. Early recognition and treatment of stump appendicitis is critical to prevent delay in diagnosis and avoid complications.
Bibliografía
- Dikicier E et al. Stump appendicitis: a retrospective review of 3130 consecutive appendectomy cases. World J Emerg Surg. 2018, 13:22. - Johnston J, et al. Stump apendicitis: surgical background, CT appearance, and imaging mimics. Emerg Radiol 2015, 22:1