Hospital: Hospital Clínico Universitario de Santiago de Compostela.
Nº: C2019-412
Aut@r o Autores: D. Machado, A. Castiñeira, P. Sucasas, M. Barrios, J. Martinez.
Presentación
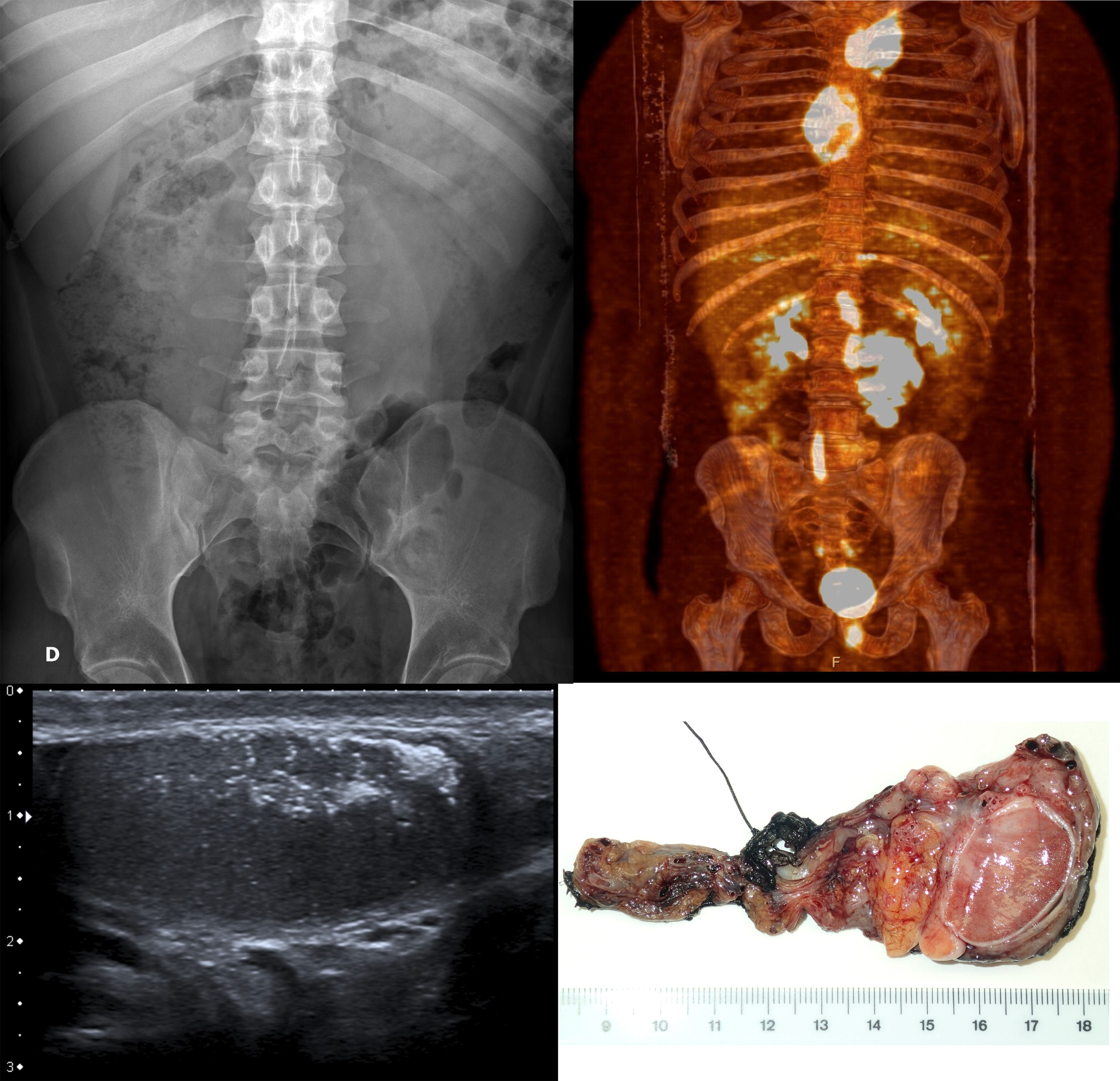
A 31-year-old man was attended at the ER in University Hospital of Santiago de Compostela due to treatment-resistant left lumbar pain, being labeled as renal colic. The blood and urine tests were normal and the abdomen Rx showed a left paravertebral mass. An ultrasound scan was performed (to complete the study) which evidenced conglomerate retroperitoneal lymph node masses. Prior to patient admission a chest x-ray was performed which was suggestive of mediastinal widening. After admittance, CT scan for thorax-abdomen and pelvis confirmed the presence of multiple mediastinal and retroperitoneal left predominant adenopathies, suggesting a germinal tumor or lymphoma as the most likely diagnosis. Testicular ultrasound was performed and the findings were highly suggestive of left germ cell testicular "burned out" tumor. Finally, a left supraclavicular adenopathy biopsy confirmed the diagnosis. The patient was treated with chemotherapy and left orchiectomy and nowadays he’s clinically disease-free.
Discusión
Testicular cancer is the most common solid malignancy affecting males between 15 and 35 years old and one of the most curable of solid neoplasms. Two broad categories of testis tumors are recognized: pure seminoma and nonseminomatous germ cell tumors. The ratio of seminoma to NSGCT is approximately one. 50 percent of this tumors, if untreated, develop "invasive" tumors within five years and 70 percent within seven years, this makes mandatory the need of early diagnosis. Seldom cases of ‘burned out’ CIS have been reported. A germ cell tumor presumably "burns out" or regresses when it outstrips its blood supply or as an immune response. Nonseminomatous germ cell tumors have the highest rate of regression. Retroperitoneal lymphadenopathy poses the following differential diagnosis: infectious, reactive, drug induced, neoplastic. After reviewing our patient’s medical history and imaging findings, the most likely diagnosis would be neoplastic (testicular cancer or lymphoma). The anatomical distribution of lymph nodes led us to testicular cancer as the most probable diagnosis and the anatopathological report confirmed our suspicion.
Conclusión
We should not underestimate simple x-ray exam in ER departments. It was the first step in the systematic radiologic approach of our patient and it allowed us the better use of alternative techniques such as US, CT, US-guided biopsy and PET. The increasingly importance of the radiologist’s role in prompt diagnosis and treatment of many diseases remains clear in our case-study and it frequently provides the best opportunity to cure.
Bibliografía
- Matilla RM, Flores MJ, Breval F. Correlación radiopatológica de los tumores testiculares en el adulto: revisión de doce casos. SERAM 2014, S-1065. Albers P, Albrecht W, Algaba F, et al. Guidelines on Testicular Cancer: 2015 Update.E