Hospital: Hospital Clínico Universitario Virgen de la Arrixaca.
Nº: C2019-452
Aut@r o Autores: I. Sánchez-Serrano, A. Cuélliga González, A. Navarro Baño, M. Martínez Cutillas, A. Castillo García, D. Gea Martos.
Presentación
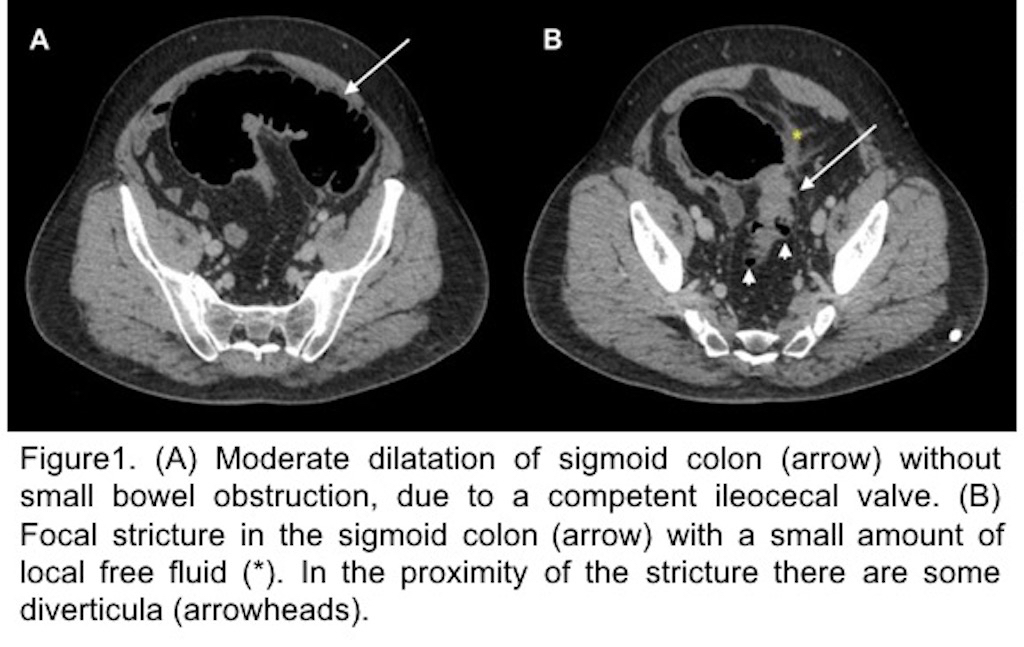
45 years old man with acute pain in the left iliac fossa for 12 hours. The abdominal examination revealed pain, involuntary rigidity and rebound tenderness in the right iliac fossa. The patient had previous clinical history of diverticulitis but he referred this episode was worse than previous ones. A CT showed isolated moderate dilatation of colon with collapse of the small bowel, and a short segment of sigmoid colon with wall thickening and stenosis. A little amount of local free fluid and some nodes were observed.
Discusión
Diverticular disease is an uncommon cause of large bowel obstruction (LBO), be shown at approximately 10-12% of cases. During an acute episode of diverticulitis, it may be caused by a bowel wall edema and pericolic inflammation, which even can cause a small bowel obstruction. High-grade obstruction is uncommon, and it is frequently caused by colorectal carcinoma. However, multiple episodes of diverticulitis can lead to fibrosis and a stricture of the wall and cause LBO [1]. The most frequent location is the sigmoid, whereas obstruction of the transverse or right colon due to diverticulitis is rare. Main differential diagnosis may be made with a colorectal carcinoma. When wall thickening affects a short segment of colonic wall (< 10 cm) and there are regional lymph nodes, colonic malignancy may be suggested. By contrast, diverticulitis usually affects a longer segment (>10 cm) with symmetric bowel wall thickening, hyperemia and presence of diverticula. In some cases, it is impossible to distinguish between diverticulitis and a colonic malignancy without colonoscopy with biopsy [1, 2].
Conclusión
Large bowel obstruction secondary to chronic diverticulitis is an uncommon cause of bowel obstruction. The importance of knowing about this entity is to make a properly diagnose and rule out others entities like colorectal carcinoma.
Bibliografía
- Jaffe T, Thompson WM. Large-Bowel Obstruction in the Adult: Classic Radiographic and CT Findings, Etiology, and Mimics. Radiology. 2015,275(3):650-62. doi: 10.1148/radiol.2015140916 - Gore RM, Silvers RI, Thakrar KH, Wenzke DR, Mehta UK, Newmark GM, et