Hospital: Hospital Universitario La Paz.
Nº: C2019-499
Aut@r o Autores: R. Alonso.
Presentación
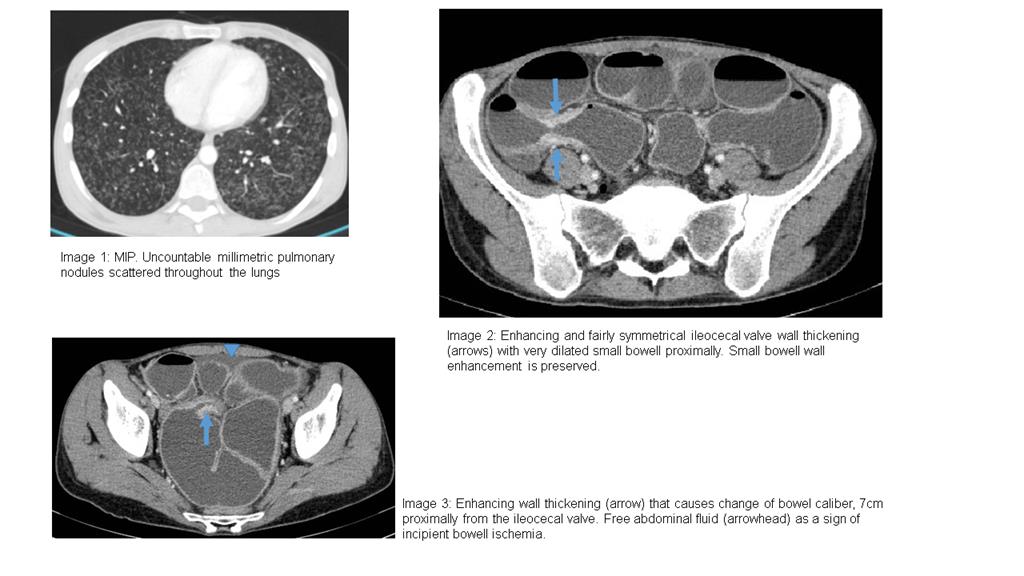
: A 32 year old female that had been admitted to another clinical center for multiresistent tuberculosis treatment was transferred to our Emergency Department for CT examination, with a short history of abdominal pain and distension. Intravenous contrast enhanced abdominopelvic CT showed the existence of small bowel mechanical obstruction, enhancing wall thickening of the ileocecal valve (that caused change in caliber) and signs of incipient bowel ischemia. Another enhancing wall thickening that caused change of bowel caliber was discovered 7cm proximally from the ileocecal valve. Low density center lymph nodes of small size were also seen in the ileocolic area. Furthermore, miliar pulmonary tuberculosis findings were observed and, therefore, a very probable diagnose of intestinal tuberculosis was reached. In this context, surgery was performed and 30 cm of small bowel was resected.
Discusión
Miliary tuberculosis is an uncommon pulmonary manifestation of tuberculosis. It represents haematogeneous dissemination of uncontrolled tuberculous infection and carries a relatively poor prognosis. It is seen both in primary and post-primary tuberculosis and may be associated with tuberculous infection in others organs. The gastrointestinal tract accounts for the sixth most frequent site of extrapulmonary involvement. Although it can involve any gastrointestinal tract segment, the ileocecal region is the most common area of involvement (90 %) due to the abundance of lymphoid tissue. Characteristic CT features include the characteristic appearance of asymetric thickening of ileocaecal valve and medial caecum and large heterogenous lymph node mass with adherent bowel loops and mesentery. Low density centre caseating nodes may be seen with minimal/no change in mesenteric fat. Despite the fact that in our case the ileocecal valve wall thickening was fairly symmetrical and in spite of lacking mesenteric lymph nodes of considerable size, the site of affection (ileocecal region) and its characteristic wall thickening in the terminal ileum made the diagnose of intestinal tuberculosis very likely. Even more so in the context of the coexisting pulmonary findings. Moreover, the bowel obstruction with incipient bowel ischemia (observed as free abdominal fluid) made the prompt surgical approach crucial in the acute process management.
Conclusión
o sum up, main imaging findings of intestinal tuberculosis include circumferential wall thickening of terminal ileum and cecum, asymmetric thickening of the ileocecal valve and mesenteric lymphadenopathy with central low attenuation areas with coexisting involvement of other organs (specially the lungs). Bowel obstruction is the most common complication requiring early surgical intervention.
Bibliografía
- Lee WK, Van Tonder F, Tartaglia CJ, Dagia C, Cazzato RL, Duddalwar VA et al. CT appearances of abdominal tuberculosis. Clinical Radiology 2012, 67(6):596-604 - Burrill J, Williams CJ, Bain G, Conder G, Hine AL, Misra RR. Tuberculosis: A Radiologic R