Hospital: Complejo Hospitalario Insular Materno Infantil.
Nº: C2019-181
Aut@r o Autores: A. Moujir Sánchez, M. González Domínguez, D. Riol Sancho, J. López Déniz, S. Lorenzo Santana.
Presentación
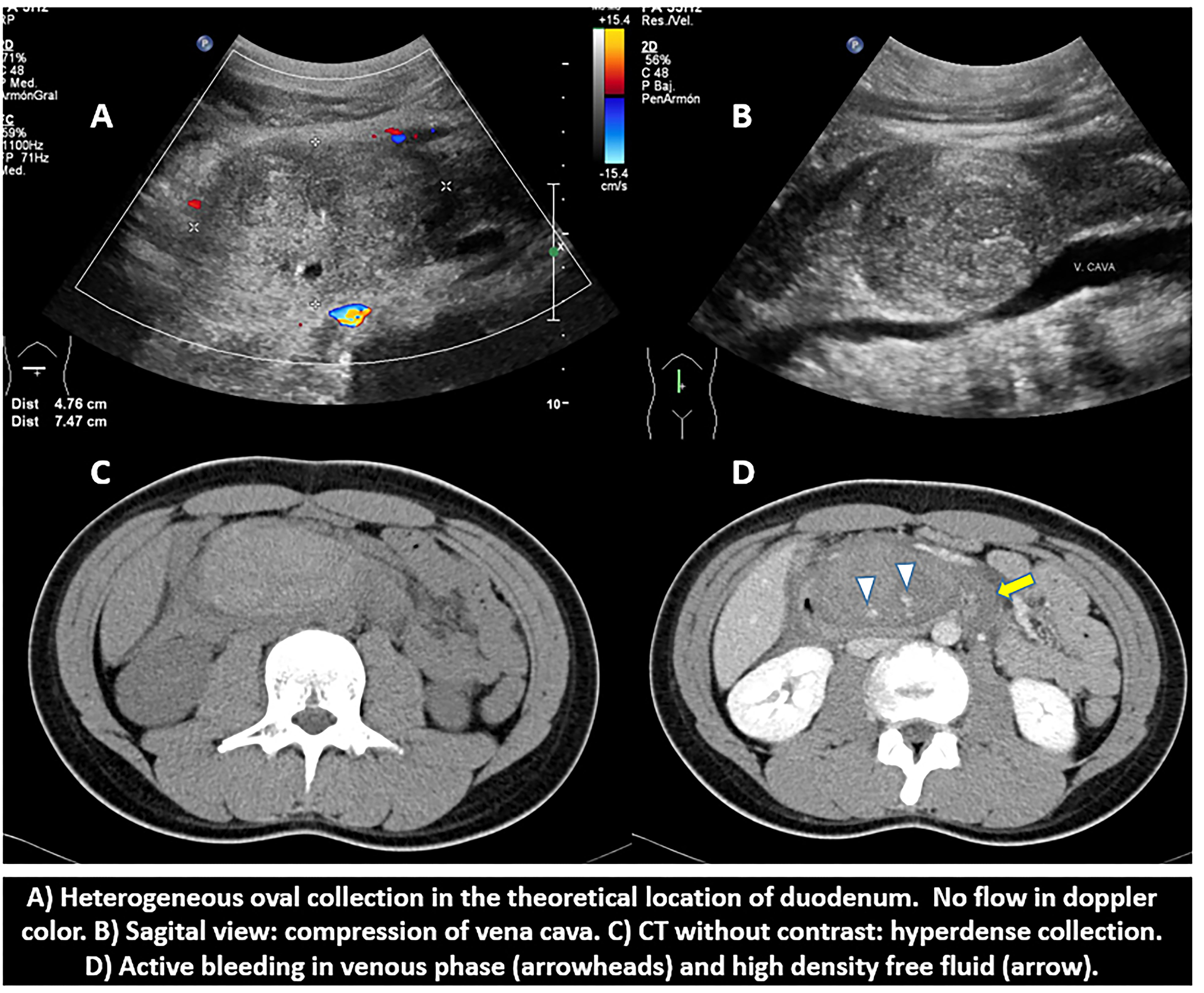
A 16 year old male comes to our emergency department due to pain and persistent vomiting after an abdominal trauma with the handlebar of a bicycle. On physical examination epigastric tenderness was noted. However there were no signs of hypovolemia or anemia (Blood pressure: 131/79 mmHg, Heart rate: 65 bpm, Oxygen saturation: 100%, Hemoglobin: 12 g/dl). A leukocytosis of 17,900/µl was the only alteration in the hemogram. Ultrasound study identified an heterogeneous oval collection in the theoretical location of the third duodenal portion. Doppler study did not showed internal vacularization (Image A). The lesion also compressed partially the inferior vena cava (Image B). Pancreas had a normal appeareance. On CT, the described lesion corresponded to an hyperdense collection (49 x 85 x 88 mm) in the third duodenal portion, in relation to a duodenal hematoma (Image C). After contrast administration, it showed no enhancement, but two points of active bleeding were observed on the venous phase (Image D). In addition, the presence of high density fluid in the anterior pararenal space was observed, in relation to hemo-retroperitoneum. No extraluminal gas was identified. Pancreas and other abdominal viscera did not showed remarkable findings. Given the hemodynamic stability, a non-interventional treatment (compression) was decided, with a favorable evolution of the patient.
Discusión
Duodenal hematomas develop in the intestinal loop wall and are usually the expression of a blunt abdominal trauma or are even spontaneous (anticoagulated patients, pancreatitis, chemotherapy…). Duodenum is predisposed to damage in traumas due to its position just anterior to the vertebral spine and its peritoneal fixation. Radiologically main signs that we must take on mind are: collection or focal thickening of intestinal wall with an ecogenic/hyperdense appearance, absence of peristalsis or free fluid. Even they are unspecific, it should be considered in an adecuate clinical context. Oral contrast is not necessary, and if used, water is preferred. Positive oral contrast can difficult diagnosis. The presence of extraluminal gas or extravasation of oral contrast will make us think about the diagnosis of duodenal perforation, which is the main differential diagnosis. However, radiologically it can present in an identical way to the duodenal hematoma, so if there are still doubts of a possible perforation, an exploratory laparotomy may be indicated. Other diagnosis that should be taken on mind are intestinal isquemia, infectious colitis and neoplasias.
Conclusión
Duodenal hematoma should be taken on mind in blunt abdominal traumas, withoutforgeting main differential diagnosis such as duodenal perforation.
Bibliografía
- Azcón FM, Martínez A y Santiago A. Hematoma intramural intestinal espontáneo: espectro de presentación y diagnóstico por imagen. Póster SERAM 2014 / S-0168 - Kunin JR, Korobkin M, Ellis JH, Francis IR, Kane NM