Hospital: Hospital Universitario Ramón y Cajal.
Nº: C2019-146
Aut@r o Autores: L. González-Campo, R.E. Pacios Blanco, M.I. García Gómez Muriel, D. Lourido García, C. Suevos Ballesteros, J. Vidal Mondéjar.
Presentación
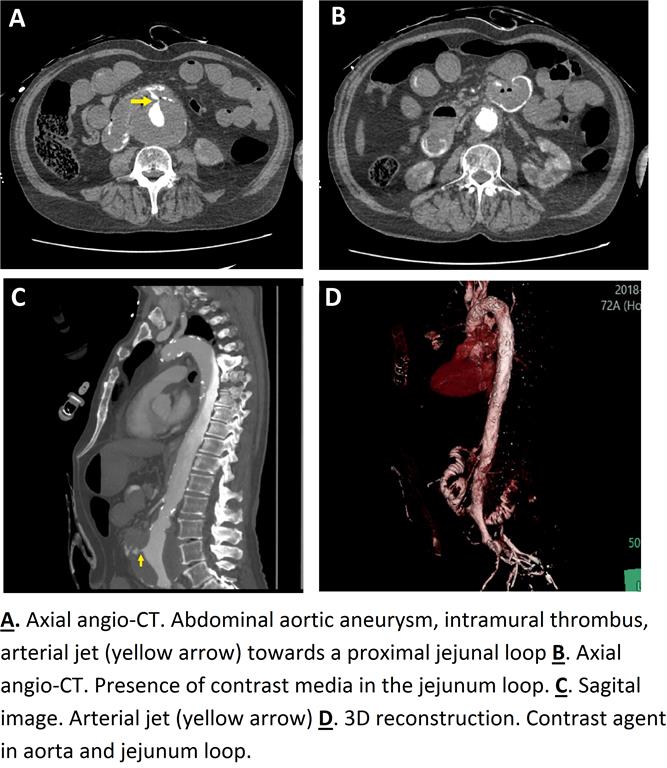
A 72-year-old male was brought to the emergency department after presenting hematemesis of roughly 500 ml and loss of consciousness. In his assessment, the most noticeably observed initially was, obtundation, pain in the lumbar region, signs of hypoperfusion and increased abdominal noises. Gastric perforation, aortic dissection and aorto-enteric fistula were considered as initial possibilities. POCUS (point-of-care ultrasound) was performed, showing dilatation of the abdominal aorta. Angio-CT of the abdominal region was requested. It showed an abdominal aortic aneurysm at the origin of the renal arteries, intramural thrombus, arterial jet towards a proximal jejunal loop and presence of contrast agent in the jejunum loop, the duodenum and the gastric cavity. The radiological diagnosis was aorto-enteric fistula. High-risk surgery was performed by the Vascular Surgery Service. Torpid evolution after surgery with generalized multiorgan failure and hemodynamic shock. Exitus
Discusión
Aorto-enteric fistulas (AEF) are the communication between the aorta and the digestive tract. Although they are rarely the cause of gastrointestinal bleeding, an early diagnosis is essential due to its high mortality rate (>75%)[1]. Autopsy studies have shown that around 3.5% of episodes of massive upper gastrointestinal bleeding are due to primary AEF. There are two groups: Primary (incidence about 0,04 – 0,07%), a consequence of aortic pathologies (90% aneurysms) or pathologies of the adjacent bowel (80% duodenum) and secondary (incidence about 0,6-2%), due to predisposing factors such as vascular prostheses, foreign bodies, traumatism, etc [2,3]. The classic clinical triad of presentation of AEF, (abdominal pain and lumbar irradiation, abdominal pulsatile mass and intestinal bleeding) is usually incomplete. The most frequent CT findings are gas inside or adjacent to the aorta, loss of the periaortic fatty plane, contrast medium in the digestive tract, retroperitoneal or intestinal wall hematoma. CT has a variable sensitivity (40%–90%) and specificity (33%–100%) for the diagnosis of aortoenteric fistulas [3].
Conclusión
Aorto-enteric fistula is a diagnostic challenge with high morbidity and mortality rates. If clinical suggestive signs or predisposing factors (secondary fistulas) are found, we must consider it as part of our differential diagnosis and not defer the performance of emergency CT.
Bibliografía
- Sandoval Santacruz MI, Huerta Orozco LD, Ramírez González LR, Reynaga Velázquez JG, Rodríguez Wohler CL, Godoy Castro VM. Fístula aortoentérica como causa de sangrado gastrointestinal masivo: diagnóstico