
Hospital: Hospital Universitario Nuestra Señora de Candelaria.
Nº: C2019-295
Aut@r o Autores: S. Benítez Rivero, C. Marichal Hernández, J. Díaz Gutiérrez, M. Fdez. Del Castillo Ascanio, Y. El Khatib Ghzal, V. Pantoja Ortiz.
Presentación
A 63-year-old male patient with a car accident, suffering a frontal collision. The patient complained of thoracic pain, with no additional symptomatology. He was hemodynamically stable. Axial contrast-enhanced CT scan showed a post traumatic contained pseudoaneurysm in the aortic isthmus, 2.5 cm distal to the origin of the left subclavian artery, associated to an extensive periaortic hematoma in direct continuity with the wall of the descending thoracic aorta. Additional CT findings included bilateral rib fractures and right lung contusion. The brain, neck and abdominal CT findings were unremarkable.
Discusión
Acute traumatic aortic injury (ATAI) is a critical life-threatening event with a substantial morbility and mortality, requiring a prompt diagnosis and management. Of all cases of blunt trauma resulting in substantial injury to the thorax, motor vehicle collisions account for a majority. In a stable patient, multidetector CT is the diagnostic test of choice. Thoracic aortic injury is the most frequent type of ATAI. The aortic isthmus is the most common location due to its relatively immobile position within the thorax. The severity of injury at this location may range from minimal intimal injury to frank rupture with active extravasation. Direct signs of ATAI include an intimal flap, traumatic pseudoaneurysm, intraluminal mural thrombus, abnormal aortic contour, and sudden change in aortic caliber (aortic “pseudocoarctation”). Rarely, a true dissection may occur. Frank aortic rupture with active extravasation is also exceedingly rare. Injuries that only involve the intima are classified as minimal aortic injuries. Indirect signs of aortic injury include mediastinal hematoma and aortic parietal hematoma (periaortic hematoma). However, periaortic hematoma is much more suggestive of aortic injury than isolated mediastinal hematoma that does not affect the periaortic fat plane.?
Conclusión
Multidetector CT is the diagnostic modality for the evaluation and accurate diagnosis of thoracic trauma. In patients with unequivocal evidence of aortic injury no further imaging is necessary. It is essential for the radiologists to be aware of the wide range ofpresentations and the various imaging findings, considering that ATAI is a lifethreatening condition with a high morbility and mortality.
Bibliografía
- Steenburg SD, Ravenel JG, Ikonomidis JS, Schönholz C, Reeves S. Acute Traumatic Aortic Injury: Imaging Evaluation and Management. Radiology 2008, 248: 748-762. - Yahia DA, Bouvier A, Nedelcu C, Urdulashvili M, Thouveny F, Ridereau C, et al. Imaging of
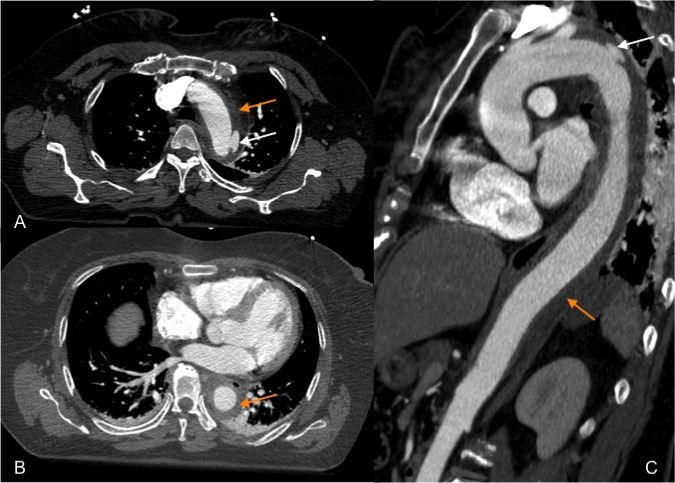
(A, B) Axial thoracic contrast-enhanced CT shows a post traumatic contained pseudoaneurysm at the level of the aortic isthmus, distal to the origin of the left subclavian artery (white arrow), with an extensive periaortic hematoma in direct continuity with the wall of the descending thoracic aorta (orange arrow). (C) Sagittal contrast-enhanced CT reformation shows the pseudoaneurysm (white arrow) and the craniocaudal extension of the periaortic hematoma (orange arrow).