Hospital: General University Hospital of Guadalajara
Nº: C2019-176
Aut@r o Autores: L. Gil, I. Zabala, B. Sastre, J. Martinez, C. Marco.
Presentación
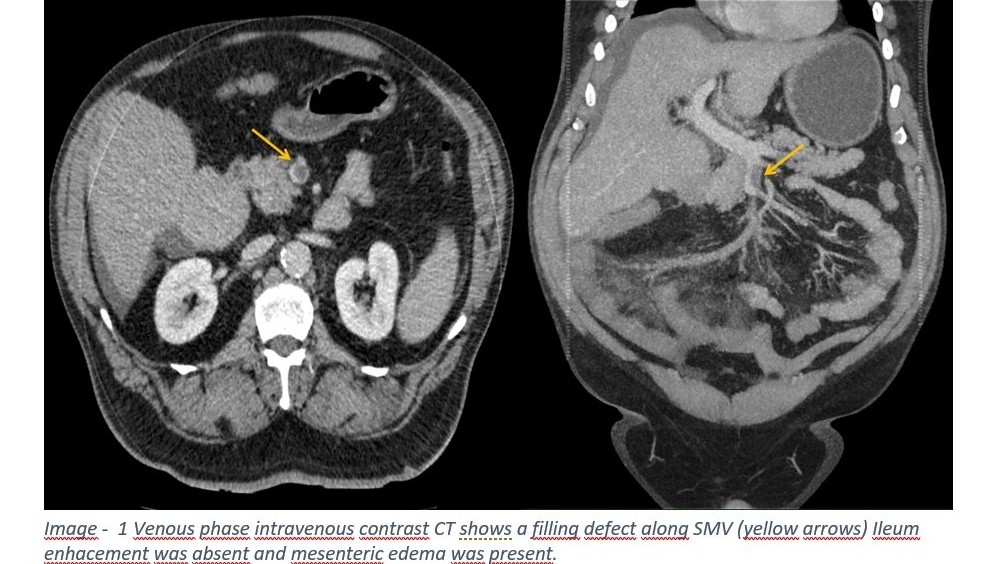
A 61 year-old male presented to the emergency room with acute upper abdominal pain irradiated to central abdomen for two days. He described diarrhoea with blood stools. He denied fever, nausea, vomiting or any urinary symptoms. Past medical history is significant for overweight, alcohol dependence, tobacco use, pulmonary thromboembolism, diabetes type 2 and coagulation profile essentially normal. The exam was normal except for intense diaphoresis and deep epigastric tenderness without signs of peritonitis. Contrast-enhanced CT revealed a filling defect in SMV extended to peripheral ileal veins. Bowel wall enhancement was absent and mesenteric edema was present. The patient was admitted under surgical service and practiced exploratory laparotomy which revealed 2.2 meters of ischaemic small bowel without evidence of perforation.
Discusión
Acute superior mesenteric vein thrombosis is a rare condition that may associate small bowel ischemia. Compared to other causes of mesenteric ischemia, acute superior mesenteric vein thrombosis accounts for 5 - 15% of all cases. The vast majority of cases are due to an underlying condition including hipercoagulable states, portal hypertension, intraabdominal or systemic sepsis, recent abdominal surgery or mechanical narrowing due to adjacent malignancy. Approximately 20% - 40% patients have past medical history of deep vein thrombosis or known hereditary hipercoagulable state. Acute superior vein thrombosis most frequently presented as abdominal pain with gradually worsening. Also can associate nausea or vomiting, fever, diarrhea and blood stools. Blood stools indicate bowel ischemia or infarction. Abdominal CT with multiple contrast phases is the test of choice. It is highly recommended to obtain non-contrast phase, arterial phase triggered when abdominal aorta reaches >100 HU and portal venous phase. The findings usually include venous filling defect, mesenteric stranding and thickening bowel wall. Management could be either medical or surgical. In early stages conservative treatment with anticoagulation, bowel rest and monitoring of clinical deterioration is prefered. Note that surgical exploration is required when there is clinical, radiological or laboratory evidence of bowel infarction or peritonitis.
Conclusión
Acute mesenteric vein thrombosis is a rare but life threatening condition that can lead to small bowel ischemia. It is important to consider in any patient with risk factors presented with unrelenting abdominal pain. Early diagnosis and treatment could avoid progression to mesenterich ischemia lowering mortality rate.
Bibliografía
- Furukawa A, Kanasaki S, Kono N et-al. CT diagnosis of acute mesenteric ischemia from various causes. AJR Am J Roentgenol. 2009,192 (2): 408-16. 2. - Warshauer DM, Lee JK, Mauro MA et-al. Superior mesenteric vein thrombosis with radiologically occult ca