Hospital: Hospital Clinico San Carlos.
Nº: C2019-588
Aut@r o Autores: C. Arizaga Ramirez, A. Mañas Hernandez, L. Sanz Canalejas, A. Nava Muñoz, M. Bertolez Cue.
Presentación
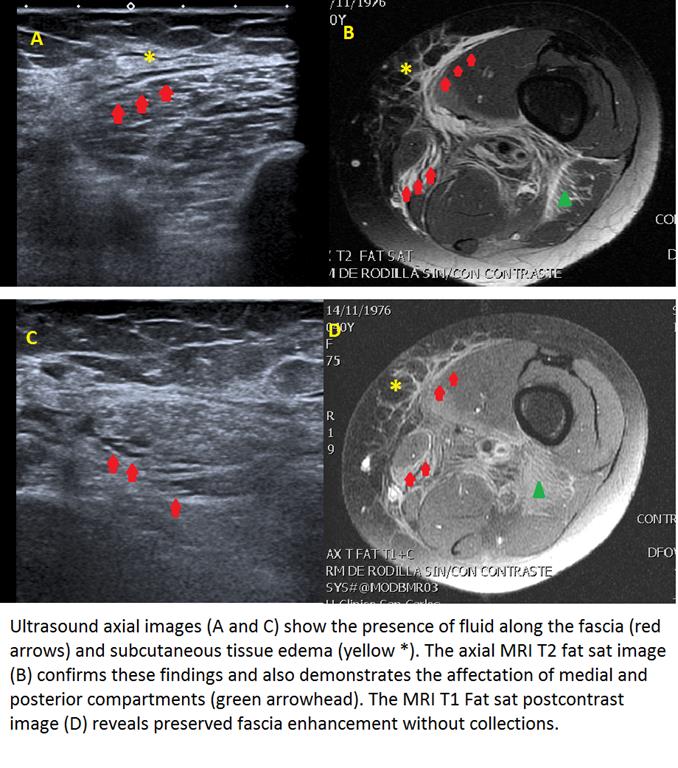
A 40 year old woman, with no clinical history, was admitted to the emergency room with fever and a painful, edematous, weak lower limb. The inner side of her thigh showed a non-elevated erythematous rash. She denied traumatisms, wounds or insect bites. Initially, a Doppler ultrasound was ordered to rule out deep vein thrombosis (DVT). However, below the point of cutaneous erythema, subcutaneous edema and deep interfascial fluid was detected. No hyperechogenic foci suggestive of gas was visualized. Given these findings, the diagnosis of fasciitis was proposed and a magnetic resonance imaging (MRI) was then recommended. MRI confirmed edema and inflammation of the posteromedial muscular compartments of the thigh, with preserved fascia enhancement and without collections. These findings suggested a non-gas producing necrotizing fasciitis. Subsequently the patient developed coagulopathy, hypotension and tachycardia. She required three debridement surgeries, antibiotic therapy and a prolonged hospital admission. Finally, Streptococcus Pyogenes was isolated.
Discusión
Necrotizing fasciitis is a rapidly progressive infection of the fascia with a significant morbidity and mortality. Its diagnosis and early intervention are essential. The initial cutaneous manifestations can be subtle evolving in advanced stages to blisters, eruptions and necrosis, with or without crepitation. It can be polymicrobial (type 1), in most cases (70-80%), due to aerobic and anaerobic germs that may or may not produce gas, or monomicrobial (type 2) caused by grampositive cocci non-gas producers, mostly Streptococcus Pyogenes. Type 2 (30%) affects individuals with no risk factors, is more aggressive due to protease production and usually entails delay in diagnosis due to clinical-analytical discordance and absence of gas visualization. In this case, ultrasound not only helped to rule out DVT but also contributed to give an initial clinical suspicion. A CT would have been the next imaging tool to perform in case of having visualized gas, however, in non-gas necrotizing fasciitis only demonstrates nonspecific inflammatory findings. Therefore MRI was the technique ofchoice because it defines more precisely the affectation of soft tissue compartments in order to determine the specific surgical approach.
Conclusión
Necrotizing fasciitis is a life-threatening disease if is not urgently diagnosed. In an important number of cases air tracking along fascial planes is not present, thus normal plain X-ray films or CT do not rule out the existence of fasciitis being necessary to perform an urgent MRI. Our case also demonstrates the importance of being aware of soft tissue ultrasound findings in order to suspect an initial diagnose and consequently order the appropriate imaging techniques such as urgent MRI in non-gas producing fasciitis. (1)
Bibliografía
- Bonne SL, Kadri SS. Evaluation and Management of Necrotizing Soft Tissue Infections. Infect Dis Clin North Am, 2017, 31(3):497–511.