Hospital: Hospital Universitario Araba.
Nº: C2019-512
Aut@r o Autores: R. González Serrano, A. Valero Macià, E. Diez Lasheras, L. Alonso Irigaray, O. Ostapenko, G.A. Finol.
Presentación
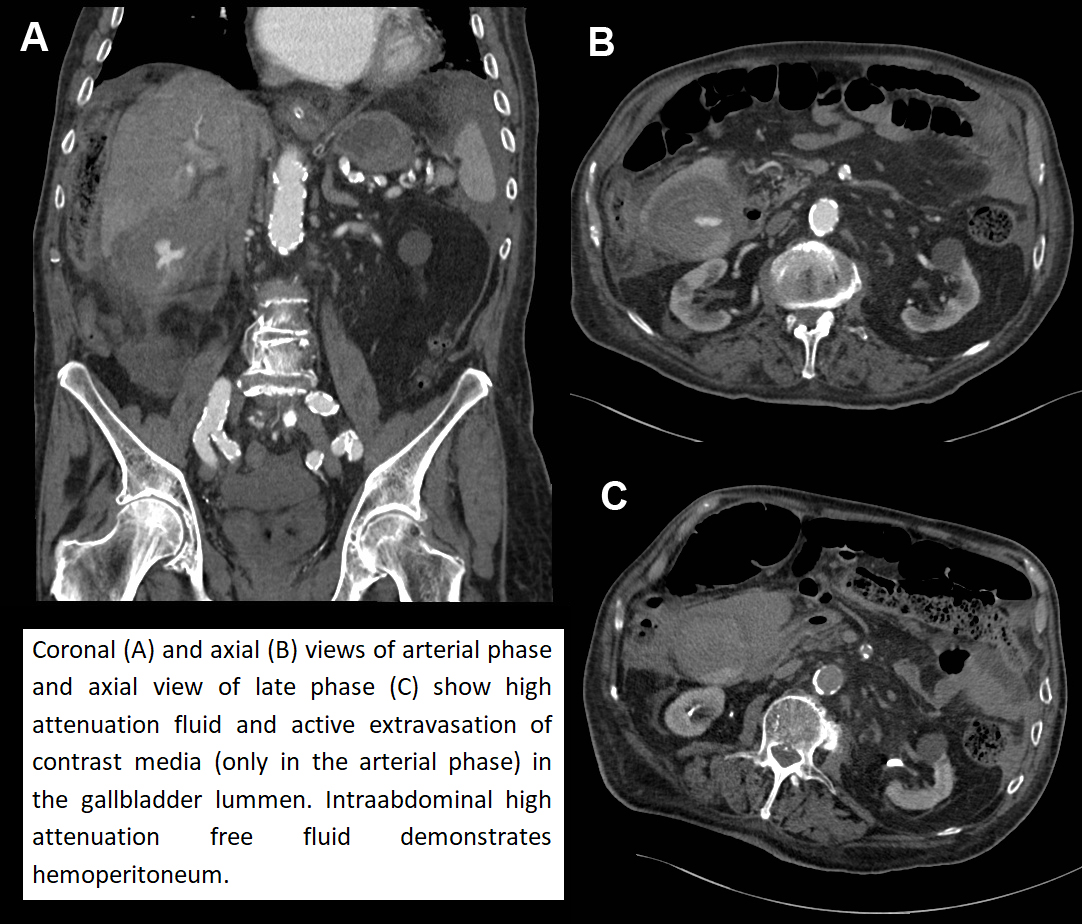
A 90-years-old male with multiple pathologies, including anticoagulated atrial fibrillation, was brought to the emergency room with an insidious clinical picture of several days with low fever and malaise. Physical examination showed abdominal distension and mild epigastric pain. Blood tests showed elevated C-reactive protein, leukocytosis with neutrophilia, thrombocytopenia and INR out of range (4.98). On computed tomography an acalculous wall-thickened gallbladder with active extravasation of contrast into the lumen suggested hemorrhagic cholecystitis. In addition, intraabdominal high attenuation free fluid was highly suggestive of gallbladder perforation and hemoperitoneum. Given patient's comorbidities conservative treatment with antibiotic therapy was chosen, prioritizing comfort measures. Despite the poor prognosis, the patient evolved favorably and was discharged 16 days after admission.
Discusión
Hemorrhagic cholecystitis is a rare but serious complication of acute cholecystitis, with a high mortality rate. Mosts cases are associated with cholelithiasis, being acalculous hemorrhagic cholecystitis quite uncommon. Physiopathologically, hemorrhage results from mucosal ulceration and/or wall necrosis secondary to inflammation. It may be easily overlooked as its symptoms mimic other more common hepatobiliary diseases. Ultrasound is usually performed due to acute cholecystitis is the first pathology suspected. In the acute phase, hemorrhage is seen homogeneous and can be confused with sludge. In later phases it adquires heterogenous echogenicity and may simulate a non-shadowing echogenic mass, raising differential diagnostic with neoplasm. Contrast-enhanced CT is useful in case of diagnostic doubts and is the first choice in unstable patients. High attenuation fluid and active extravasation of contrast media in the arterial phase may be seen in the gallbladder lummen. In case of perforation CT may also show intraabdominal high attenuation free fluid, demonstrating hemoperitoneum. All of these signs were present in our case. Emergent cholecystectomy is the treatment of choice to prevent more serious complications. In non-surgical patients cholecystostomy is an option.
Conclusión
Hemorraghic cholecystitis is a rare but serious complication of acute cholecystitis, usualy not suspected in the emergency room. Both US and CT are useful to establish an early diagnosis, so surgery is not delayed in this potentially fatal disease.
Bibliografía
- Bennett GL, Balthazar EJ. Ultrasound and CT evaluation of emergent gallbladder pathology. Radiologic Clinics of North America, 2003,41(6):1203– 1216. - Tavernaraki K, Sykara A, Tavernaraki E, Chondros D, Lolis ED. Massive intra peritoneal bleeding due