Hospital: Hospital Universitario La Paz.
Nº: C2019-604
Aut@r o Autores: F. García Martínez, A. Díez Tascón, A. Barrios, M. Caicoya Boto, E. Lanz Santos, M. Martí De Gracia.
Presentación
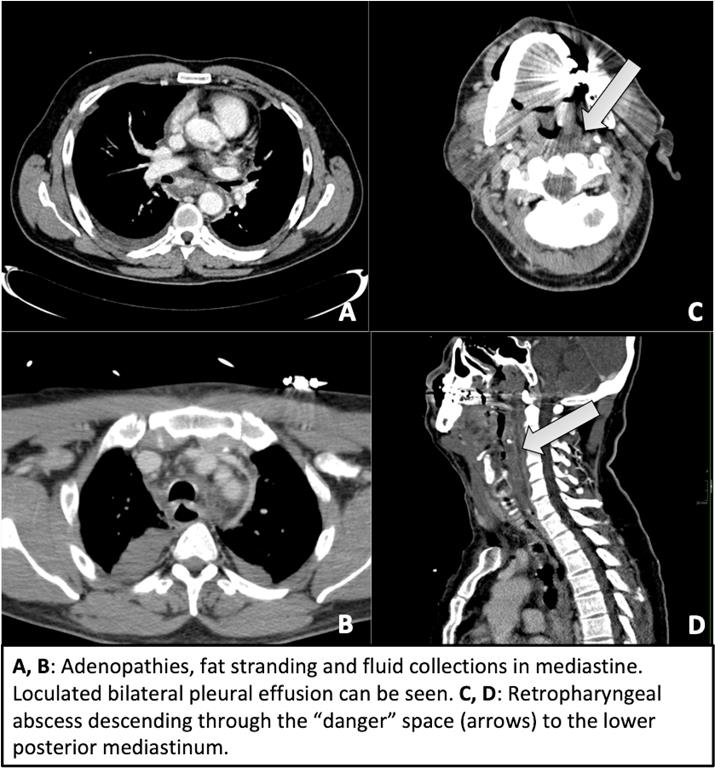
A 53-years-old male presented to the emergency department with severe abdominal pain with tenderness and peritoneal irritation in epigastrium after a 2-days history of pharyngoamigdalitis treated with antibiotics and steroids. Because of the poor general state, a perforation was suspected and an abdominal CT was performed. Abdominal structures were unremarkable but fat stranding and adenopathies in lower mediastinum and bilateral loculated pleural effusion were found. Mediastinitis was suspected and thorax and neck CT were realized showing a retropharyngeal abscess with extension to the visceral and danger spaces, leading to thyroiditis and mediastinitis, respectively. The patient underwent emergency cervicotomy and thoracotomy obtaining more than 1000 ml of purulent material from mediastinum and pleura. The patient died of multiple organ failure within 3 days despite early diagnosis and correct treatment.
Discusión
Descending necrotizing mediastinis is a rare and severe infection that occurs as a complication of an odontogenic or cervicofascial infection or cervical trauma and it is usually caused by anaerobic and aerobic bacterial of oral microbiota. The diagnosis of cervical infection is usually suspected with physical examination and clinical history, but mediastinal involvement is insidious and the delay of diagnosis is one of the primary reasons for its high mortality. It may reach the mediastinum by three pathways: the pretracheal route to the anterior mediastinum, the lateral pharyngeal route to the middle mediastinum and the retropharyngeal-retrovisceral way, which is the most common: the infection spreads into danger space, between the alar and prevertebral fasciae and drains into posterior mediastinum, resulting in mediastinitis and empyema. Multiplanar contrast enhanced CT can immediately confirm the diagnosis showing the pathway for the spread of the neck to the mediastinum. Most common findings are fluid collections, fat stranding, cellulitis, myositis or lymphadenopathies in the neck tissues and fluid collections in the mediastinum, pleura and/or pericardium, vascular thrombosis may be present. The extension should be described (above the carina, lower anterior mediastinum or lower posterior mediastinum) for correct surgery planning.
Conclusión
Descending necrotizing mediastinitis is a high mortality infection due to its aggressivity and delay of diagnosis. The history of cervicofacial infection in a critical patient should raise the alarms because of its anatomical connection, and a contrast enhanced CT must be done to confirm it and initiate early treatment.
Bibliografía
- Scaglione M, Pinto A, Giovine S, Di Nuzzo L, Giuliano V, Romano L. CT features of descending necrotizing mediastinitis: a pictorial essay. Emergency radiology. 2007,14(2): 77-81 - Papalia E, Rena O, Oliaro A, Cavallo A, Giobbe R, Casadio C, Maggi G, Ma