Hospital: Hospital Universitario Central de Asturias.
Nº: C2019-363
Aut@r o Autores: M. Blanco Guindel, G. Fernández Suárez, V. Santamaría Pérez, A. Montes García, F. García Arias, A. Fernández Del Valle.
Presentación
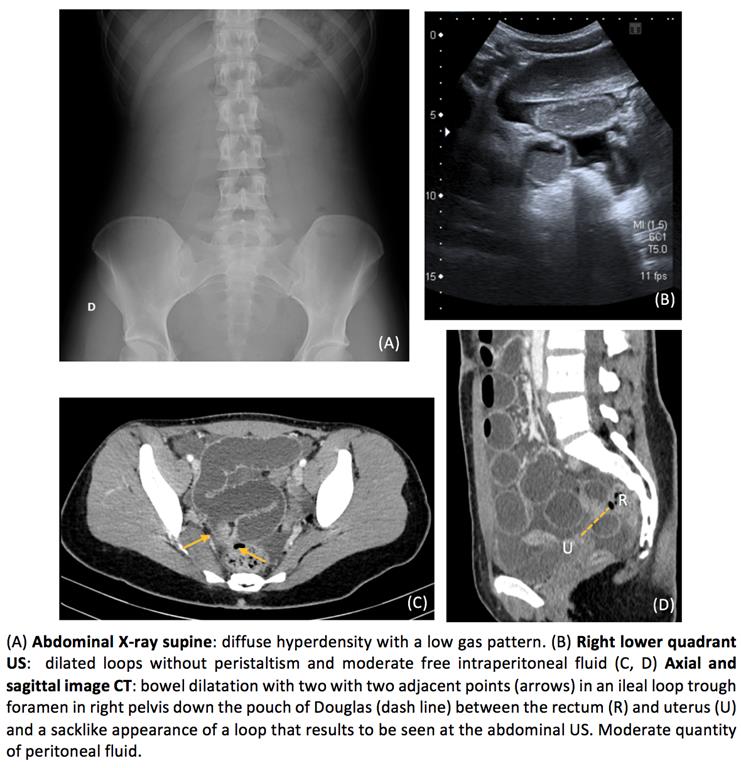
: A 20 year-old female with no history of abdominal surgery or pregnancy came to Emergency department referring abdominal pain for 3 days next to vomiting and no oral tolerance. Physical examinations confirmed abdominal tenderness. Blood test revealed leukocytosis with neutrophylia. T he abdominal X-Ray showed diffuse hyperdensity with low gas pattern. Abdominal US was performed for suspicion of appendicitis, showing dilated loops without peristaltism and moderate free intraperitoneal fluid. An abdominal MDCT was performed to confirm small-bowel obstruction (SBO), specify the cause and any complications associated. CT findings were bowel dilatation with two adjacent transition points in an ileal loop at the pouch of Douglas, which impressed enter through a hole. Surgery confirmed CT findings and evidenced a 1 centimeter peritoneal defect in the pouch of Douglas. Congenital peritoneal defect was assumed bassed on her non-surgical history.
Discusión
Internal hernias are a rare cause of SBO (0,5 - 4,1 %) due to protrusions of the viscera through peritoneum or mesentery. They are a surgical emergency that can develop into intestinal ischemia. Preoperative diagnosis is challenging, because their non specific signs and symptoms. Hernias in the pouch of Douglas are extremely infrequent. In the few reported cases in literature, some were congenital peritoneal defects and others were assumed to be secondary, depending on previous pelvic surgeries or pregnancy. Typical findings include SBO with dilated proximal loops and decompressed distal bowel. A sacklike appearence suggest and intestinal closed loop. The isolated segment is fluid filled and progressively dilated, difficulting venous return and causing ischemia. The pressence of radiological signs of bowel ischemia like wall thickening, mesenteric edema, peritoneal or mesenteric fluid, abnormal wall enhacement and pneumatosis, increasing mortality in a 25%.
Conclusión
Congenital peritoneal defects are an extremely rare cause of SBO and a potentially surgical emergency. They can often be misdiagnosed due to their non specific signs and symptoms. Familiarity with their CT findings allows an accurate and specific diagnosis.
Bibliografía
- Paulson, E.K., Thompson W.M. Review of Small-Bowel Obstruction: The Diagnosisand When to Worry. Radiology. 2017. 275 (2): 332-42. Suwa, K., Yamagata T., Hanyu K., Suzuki T., Okamoto T., Yanaga K. Internal hernia through a peritoneal defect in the pouch