Hospital: Hospital Universitario de Getafe.
Nº: C2019-716
Aut@r o Autores: E. Escudero Romo, G. Ugena Díaz, I. Cedrún Sitges, G. Íbero Díaz, T. Corbalán Sevilla, J.M. Sánchez Reyes.
Presentación
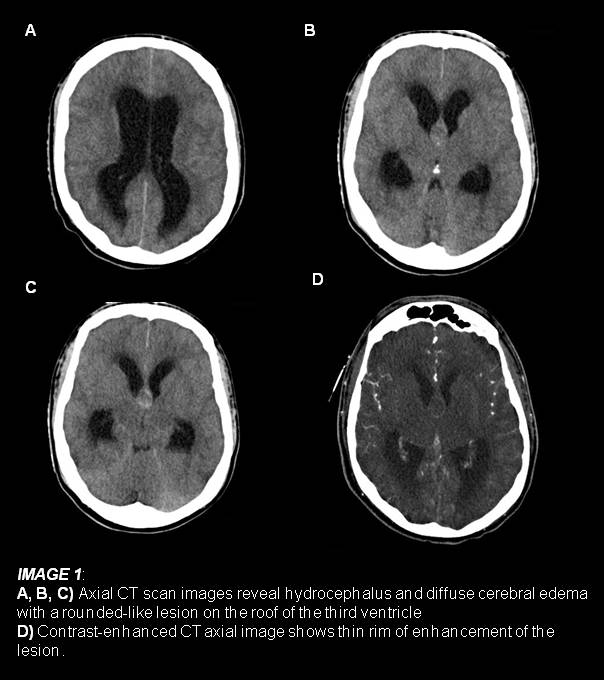
A 16-year-old male was referred to the emergency department complaining of a gradually worsening headache for the last 3 days. He described it as intermittent left hemicranial, throbbing, resistant to analgesia, associating nausea and vomit on the last 24 hours. The neurological examination revealed somnolence. An emergency non-contrast computerized tomography (CT) scan was performed to exclude acute subarachnoid hemorrhage (SAH) as the first suspected diagnosis. The CT scan reveal an heterogeneous rounded-like lesion at the roof of the third ventricle producing important hydrocephalus and effalced sulci compatible with diffuse cerebral edema. Despite some rather suggestive findings, given the proximity of the lesion to the anterior communicating artery and the initial suspicion of SAH, a contrastenhanced CT was also performed.
Discusión
Both CT findings were consistent with an obstructive colloid cyst of the third ventricle causing hydrocephalus and diffuse cerebral swelling, without signs of acute intracranial hemorrhage and an ordinary circle of Willis. Colloid cysts are benign mucin-containing tumors almost always located on the roof of the anterior side of the third cerebral ventricle, behind the foramen of Monro. They account for 0'5-2% of all intracranial primary tumors. Clinical symptoms may be intermittent and non-specific, headache being present in 68-100% of patients, characterized by its short duration and usually relieved by change in position or sleep. Other common symptoms are nausea, vomiting and visual changes. The clinical importance of these lesions is their risk to interfere with the cerebrospinal fluid outflow causing acute hydrocephalus and occasionally brain herniation with rapid clinic deterioration and even death. Note that cyst size does not appear to be a reliable predictor of outcome. The most common finding on CT scan is a rounded and smooth mass, varying in size, in most cases hyperdense, located on the anterior region of the third ventricle’s roof. After administration of contrast material, none or a thin rim of enhancement may be present. Treatment of colloid cysts includes microsurgical procedures or stereotaxic and endoscopic aspiration, among others.Based on the clinical situation and radiological findings, an emergency external ventricular drainage was inserted. Later on the patient underwent neurological resection of the lesion, with favorable evolution.
Conclusión
It’s important to prioritize and think about potentially lethal conditions such as those producing obstructive hydrocephalus. Colloid cysts are a rare but important cause of acute clinical deterioration and even sudden death, making early detection and treatment a priority. For radiologists, the imaging appearance of a colloid cyst, well-delineated hyperattenuated mass at the foramen of Monro, is almost pathognomonic.
Bibliografía
- Osborn AG, Preece MT. Intracranial cysts: radiologic-pathologic correlation and imaging approach. Radiology. 2006,239 (3): 650-64.