Hospital: Hospital Universitari de Bellvitge.
Nº: C2019-195
Aut@r o Autores: D. Pittí Freiburghaus, D.E. Nova Vaca, I. Rodríguez Caamaño, M. Pérez Rubiralta, M.M. Serra Salas, M.E. De Lama Salvador.
Presentación
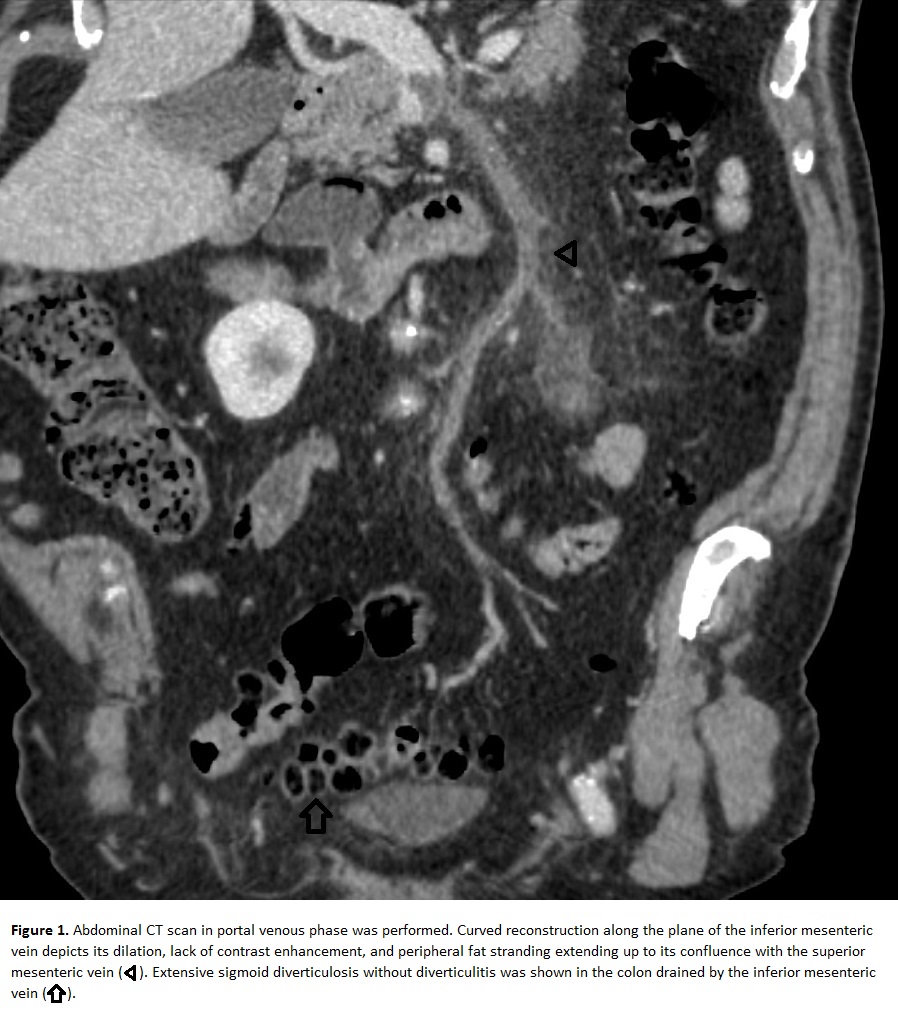
A 73-year old man with unremarkable clinical history presented to the emergency room with unspecific symptoms of mild abdominal discomfort associated with cough and rhinorrhea. In the ER basic blood tests were performed and leukocytosis (13.000/µL), neutrophilia (10.950/µL) and elevated PCR (180.6 mg/L) were shown as substantial abnormalities. The diagnosis was first suspected to be an upper respiratory tract infection, but the patient was febrile during observation and blood cultures taken were positive for gram negative bacilii which was not consistent with this diagnosis. The patient denied any other present/recent abdominal or gastrointestinal symptoms and bacteremia by Bacterioides Fragilis was proven by the blood culture. Therefore, an abdominal CT scan was performed which showed thrombosis and dilation of the inferior mesenteric vein up to its confluence with the superior mesenteric vein, as well as interstitial edema and adjacent fat stranding, findings consistent with Pylephlebitis. However, no other septic abdominal focus was found in the CT, and only extensive diverticulosis without signs of acute diverticulitis was found. Treatment was initiated with amoxicillin-clavulanate and tinzaparin with adequate response and complete resolution of the Pylephlebitis in a subsequent CT control 1 month later.
Discusión
Pylephlebitis (Septic Thrombosis) can complicate any abdominal or pelvic infection that occurs in the regions drained by the portal venous system, the most frequent causes are diverticulitis, appendicitis, cholangitis or inflammatory bowel disease. In the absence of an obvious intra abdominal septic focus, other possibilities should be considered such as coagulation alterations, malignant diseases such as hepatocellular carcinoma or acquired immunodeficiency syndrome. However, further testing in our patient ruled out these conditions.The most commonly isolated microorganism is Bacteroides fragilis, as in our case, followed by aerobic Gram-negative bacilli (E. coli, Aerobic Streptococci). Pylephlebitis clinical presentation is variable: it can occur in an almost asymptomatic patient, until severe forms complicated with septic shock with liver failure. Our patient only presented with mild abdominal discomfort.The most useful technique for its diagnosis is CT, which can show thrombosis or, less frequently, portal gas and help define the abdominal infectious focus.The management of pylephlebitis is based on broad-spectrum antibiotic therapy. Anticoagulation therapy has also proven useful.
Conclusión
In the setting of gram negative bacilii bacteriemia without remarkable abdominal symptoms, early CT scan of the abdomen proved useful in demonstrating inferior mesenteric vein pylephlebitis and early treatment prevented any complications and successful recovery. Although no obvious intraabdominal focus was present, based on the localization of the thrombosis and the extensive colonic diverticulosis, we suspect a past sub-clinical diverticulitis episode as a probable cause.
Bibliografía
Falkowski AL, Cathomas G, Zerz A, Rash H, Tarr P. Pylephlebitis of a variant mesenteric vein complicating sigmoid diverticulitis. Journal of radiology case reports. 2014,8(2):37–45