Hospital: Hospital Universitario Virgen de la Victoria., AGS Málaga Norte Hospital Comarcal de Antequera.
Nº: C2019-369
Aut@r o Autores: C. Palma González, J. Martos Fornieles, M. Carrera Martínez.
Presentación
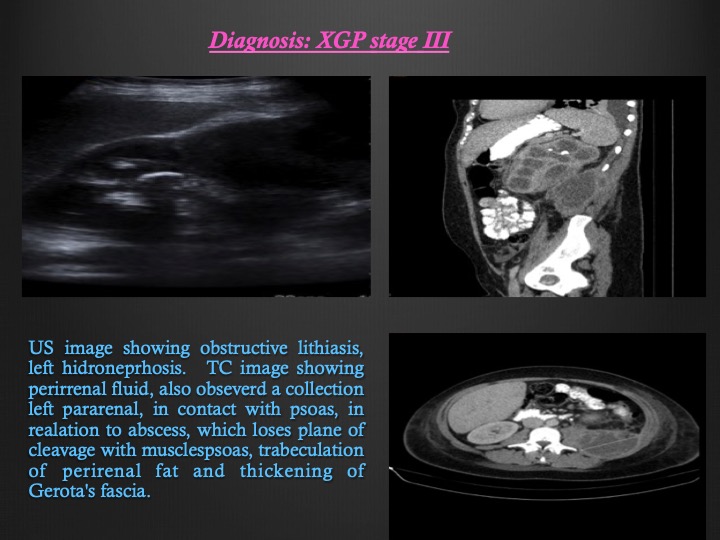
Female patient, 28 years old, admitted due to febrile syndrome, FRI pain. With leukocytosis, Hb: 8.10 mg / dl, CRP: 274. Ultrasound and urgent CT scan: Left kidney, obstructive lithiasis in a 10mm ureteropielic junction, staghorn lithiasis in the superior region and 9 mm lithiasis in the inferior region. Left hydronephrosis, pielocalicial ectasia grade IV / IV. Perirenal fluid, also observed a collection (9.4x6.4x5.4) left posterior pararenal, in contact with lower renal pole and psoas that previously displaces said kidney, in relation to hematoma vs abscess, which loses plane of cleavage with muscles psoas, trabeculation of perirenal fat and thickening of Gerota's fascia. Conservative treatment was performed (double J catheter, treatment with ATB and red blood cell transfusion) with poor response. Control CT: left pararenal collection in progress with moderate amount of free liquid in left paracolic droplet and in Douglas (new appearance). It was decided to carry out surgery: left nephrectomy. Diagnosis: XGP stage III. Postoperative without complications.
Discusión
PXG is an infrequent form of renal inflammatory disease, as a result of chronic infection of the renal parenchyma. The renal parenchyma is destroyed and replaced by lipid-filled macrophages. It is usually unilateral, it can be diffuse, focal or segmental. The most frequent form (85%) corresponds to the diffuse and unilateral form. It is usually associated with nephrolithiasis (70%), bacteriuria of the ascending urinary tract, diabetes mellitus. More frequent in women (2.1) of middle age. The majority of patients present a non-specific clinical manifestation: pain, flank mass, weight loss and UTI, (proteus or E. coli), low-grade fever. The kidney affected diffusely is not functioning. Laboratory studies: anemia, leukocytosis and elevated CRP. Imaging tests: simple abdominal radiography, intravenous urography, which show nonspecific findings although diagnostic approach, while ultrasound and CT are usually more diagnostic imaging tests in cases of PXG in its most frequent form, diffuse PXG. Ultrasonographic findings (diffuse XGP): renal hypertrophy, conservation of the reniform profile and absence of cortico-medullary differentiation that is replaced by liquid collections (dilated chalices or areas of parenchymal destruction). The renal sinus can be intensely echogenic, with extensive acoustic shadows due to coralliform calculi.
Conclusión
We should suspect it (diffuse XGP): in patients with a history of chronic renal parenchymal infections, and findings such as: parenchymal thinning, hydronephrosis, stones, detritus in a dilated collecting system and liquid perinephric collections. The CT is the definitivediagnostic test, since it allows to identify the existence of intrarenal pathology as well as a possible extrarenal extension of the disease. Treatment of choice is surgical: Total nephrectomy in patients with diffuse XGP.
Bibliografía
- Leoni FA, Kinleiner P, Revol M, et al. Pielonefritis xantogranulomatosa, revisión de 10 casos. Arch Esp Urol. 2009,62:259-71. - Dell´Aorivutila N, Guarino S, del Vecchio W, et al. Xanthogranulomatous pyelonephritis mimicking a renal cell carcino