Hospital: Hospital Universitario de donostia, Hospital Universitario Donostia.
Nº: C2019-487
Aut@r o Autores: V. Gomez Usabiaga, G. Arenaza Choperena, A. Ugarte Nuño, E. Garmendia Lopetegui, E. Pardo Zudaire.
Presentación
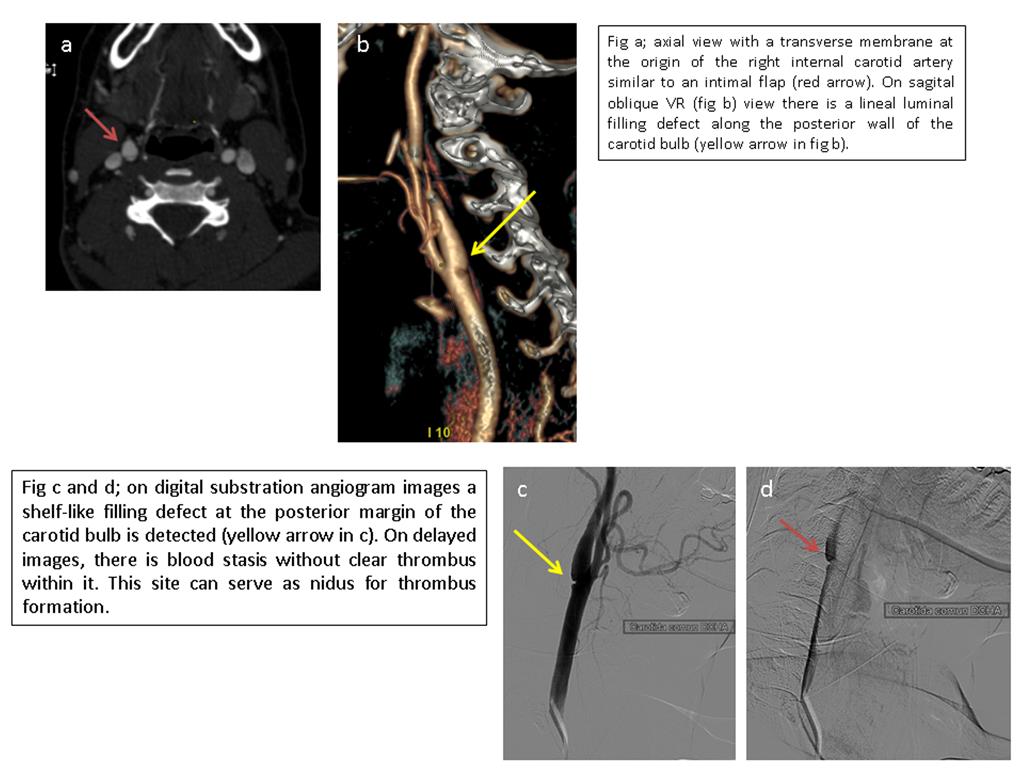
A 44-year-old female with medical history of right middle cerebral artery syndrome in 2014 presents to the emergency room in 2015 with right facial sided dysesthesia and left upper weakness partially recovered. A non-contrast CT demonstrated a right frontal encephalomalacia of the prior episode with no acute findings. The patient was treated with adiro 300mg and was discharged to a neurology facility. On DWI imaging performed 7 days later a new small cortical right frontal infarct was detected. The rest of examinations were within normal limits and the ischemic stroke was classified as crytogenic. On CTA and digital substraction angiogram images a shelf-like filling defect along the posterior margin of the right internal carotid artery origin was detected. There was no significant stenosis, nevertheless on delayed angiogram images the contrast was retained with blood stasis at that point. Finally, the patient underwent an endartherectomy and pathologist described a fibroelastic thickening of the arterial intima. The findings were consistent of a carotid web.
Discusión
Carotid web is described as focal thin, smooth, gracile, triangular in shape and membrane-like non-atherosclerotic intraluminal filling defect along the posterior wall of the internal carotid bulb. Small on size and usually non-stenotic (sagittal views are important to better visualize). On the axial view an axial septum can be seen. Histopathologically is thought to represent an intimal variant of fibromuscular dysplasia as it is characterized by fibroelastic thickening of the arterial intima. There is evidence emerging for an association of these lesions with ischemic strokes. Up to one third of patients with ischemic strokes lack of an identifiable cause. Most of these cases affect younger people with no risk factors. Carotid webs are thought to be an underdiagnosed cause of cryptogenic strokes. Some authors propose that carotid webs produce stasis of blood flow distal to the web and serve as nidus of thrombus formation which can embolize distally. Carotid webs may be distinguished from fibromusuclar dysplasia which is a segmental non-atherosclerotic and non inflamatory vascular disease, most commonly affects mid and distal portions of the internal carotid and vertebral arteries as multiple stenosis in a string-of-beads pattern, often bilaterally. Atherosclerotic plaques typically appear as concentric mural calcification or hypoattenuation with or without luminal narrowing.Finally, dissection flaps are not localised and typically propagate beyond the carotid bulb, associate mural hematoma or pseudoaneurysms. There are no current guidelines for carotid webs and optimal management is still debated. Several treatment options have been proposed especially for symptomatic webs, such as carotid endarterectomy and stent placement.
Conclusión
Carotid webs must be taken into account as a possible cause of ischemic strokes, specially in younger patients with no risk factors. Sagittal views are important not to miss subtle webs.
Bibliografía
- Wojcik K, Milburn J., Steven A. Carotid webs: Radiographic Appearance and Significance.Ochsner Journal 2018,18:115–120. - Sajedi PI, Gonzalez JN, Cronin CA, Kouo T, Steven A, Zhuo J, et al. Carotid Bulb Webs as a Cause of "Cryptogenic" Ischemic Stroke.