Hospital: Hospital Universitario La Paz.
Nº: C2019-544
Aut@r o Autores: A. Barrios, A. Diez, E. Lanz, F. García, M. Caicoya, M. Marti.
Presentación
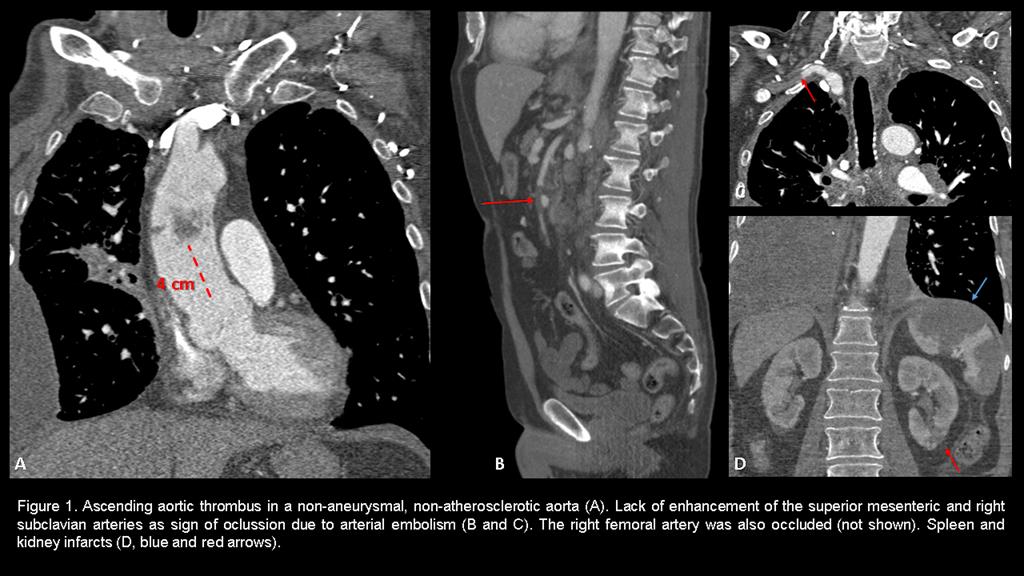
59 year-old-man, with history of advanced signet-ring cell adenocarcinoma of the lung receiving pemetrexed and carboplatin, complained of sudden onset of abdominal and right arm and leg pain. On physical examination these limbs were cold, pale and pulseless. Increased serum lactate and d-dimer levels were found on laboratory tests. A computed tomography angiography (CTA) was requested on clinical suspicion for arterial embolization (Figure 1). A transesophageal echocardiography (TTE) confirmed these findings. Endovascular thrombectomy was performed.-
Discusión
Atherosclerotic plaque-related thoracic aortic thrombus is frequently experienced by elderly patients. A thoracic aortic mobile thrombus (TAMT) in the absence of underlying atherosclerosis or aortic aneurysm is limited to small case series. The pathogenesis of TAMT is unknown, but endothelial damage caused by cytokines may trigger platelet deposition, particularly in the hypercoagulable state of advanced stage malignancies. Thrombotic episodes occur in up to 60% of patients with mucin secreting adenocarcinoma. The most common chemotherapeutic agents implicated in arterial thrombosis are platinum-based antineoplastic. Other causes include genetic, hypercoagulable, primary endothelial or iatrogenic diseases. The diagnosis is usually made after clinical manifestations of peripheral embolism. Lower limbs are the most common location (60%), followed by mesenteric emboli (18%). TEE has become the study of choice to exclude a cardioembolic source and proximal TAMT. Most TAMT are located in the descending thoracic aorta and just few cases in the ascending aorta or aortic arch. CTA should be performed in all patients, since TEE may miss thrombi because of conduction loss due to the trachea. CTA also allows the identification and exact location of the thrombus, which is helpful in planning a surgical approach and it helps to exclude aortic wall malignancy that serves as the nidus for thrombus formation. Moreover, genetic and hypercoagulability work-up should be performed. Currently, long-term anticoagulation is the most widely accepted first-line therapy. Surgery is favoured in patients with low risk of perioperative complications, those in whom conservative treatment has failed, and those who have a highly mobile thrombus and a consequently high embolic risk. Surgical options include thrombectomy, segmental aortic resection, thromboaspiration, and endoluminal stent-grafts. Stent-grafting is prefered for reestablishing vascular patency and excluding the thrombus, thus minimizing fibrin and platelet deposition.-
Conclusión
TAMT in the non-aneurysmal, non-atherosclerotic aorta is a rare cause of peripheral embolism. However, it should be considered in patient with hypercoagulable state. ETE andCTA are helpful for diagnosing and treatment approaching.-
Bibliografía
- Tigkiropoulos K, Karamanos D, Tympanidou M, Saratzis N, Lazaridis I. Aortic Arch Floating Thrombus Complicated by Distal Embolization in a Patient with Malignancy. Case Rep Vasc Med. 2018,2018:2040925. - Pagni S, Trivedi J, Ganzel B, et al. Thoracic