Hospital: HOSPITAL CLINICO SAN CARLOS.
Nº: C2019-205
Aut@r o Autores: C. Sánchez Rodríguez, A. Mañas Hernández, A. Pérez Bartolomé, C. Arizaga Ramírez, A. Vidal González
Presentación
A 31 year old man with no clinical history came to the emergency room due to progressive testicular pain after trauma. The right testicle was correctly positioned inside scrotal sac without horizontal lie. It has doubled its size and consistency, was slightly tender at papation and did present neither palpable masses nor fluctuation areas. The scrotal skin showed a superficial contained hematoma. Prehn sing was negative and the transillumination examination showed no alterations. The left testicle, penis and perineum were normal. A Doppler ultrasound was performed and revealed slightly testicular asimetry, being the right one larger with increased vascular flow. The lower pole morphology was abnormal due to a discontinuity of the tunica albuginea with herniation of the intratesticular content. There were also intratesticular hipoechoic regions as well as heterogeneous septate content within the testicular sac, suggestive of hematomas and haematocele and thickening of covers. All these ultrasound findings supported clinical suspicion of testicular rupture. The patient required surgical intervntion resulting in orquiectomy due to testicular lower pole complete laceration and necrosis
Discusión
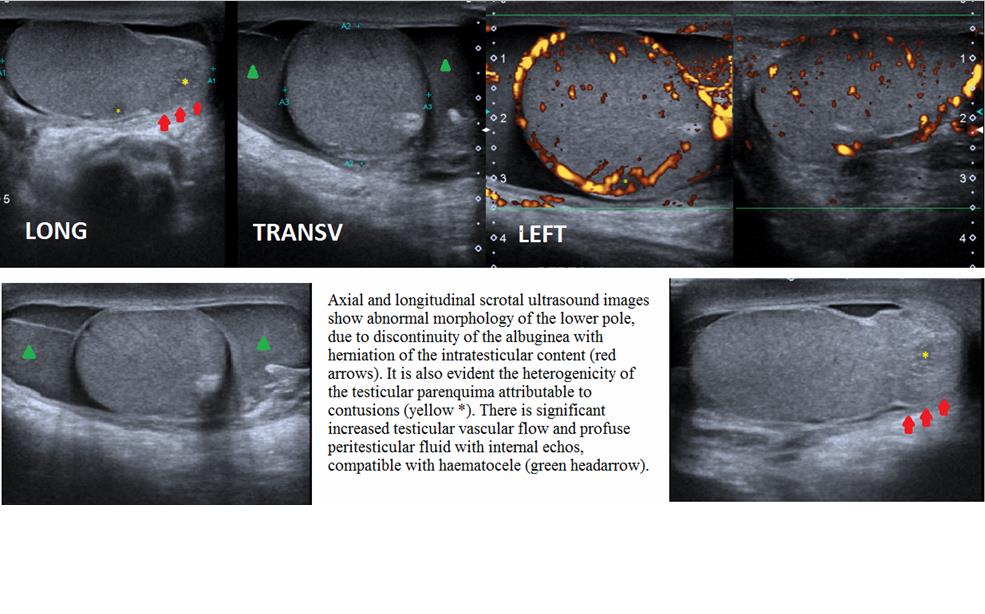
Scrotal trauma is uncommon in the emergency room. Common symptoms are pain, tenderness, skin ecchymosis and/or scrotal hematoma. Ultrasound is the modality of choice for initial evaluation, mode B is an important tool for assessing morphology, size and intra or extratesticular lesions. Color Doppler ultrasound is also useful because detects perfusion alterations and evaluation of viability prognosis. Axial and longitudinal scrotal ultrasound images show abnormal morphology of the lower pole, due to discontinuity of the albuginea with herniation of the intratesticular content (red arrows). It is also evident the heterogenicity of the testicular parenquima attributable to contusions (yellow*). There is significant increased testicular vascularflow and profuse peritesticular fluid with internal echos, compatible with haematocele (green headarrow). Findings suggestive of testicular rupture are: