Hospital: Complejo Hospitalario Insular Materno Infantil.
Nº: C2019-215
Aut@r o Autores: A. Moujir Sánchez, E. Cevallos Castañeda, D. Riol Sancho, M. González Domínguez, A. Uriarte Rodríguez, J. López Déniz.
Presentación
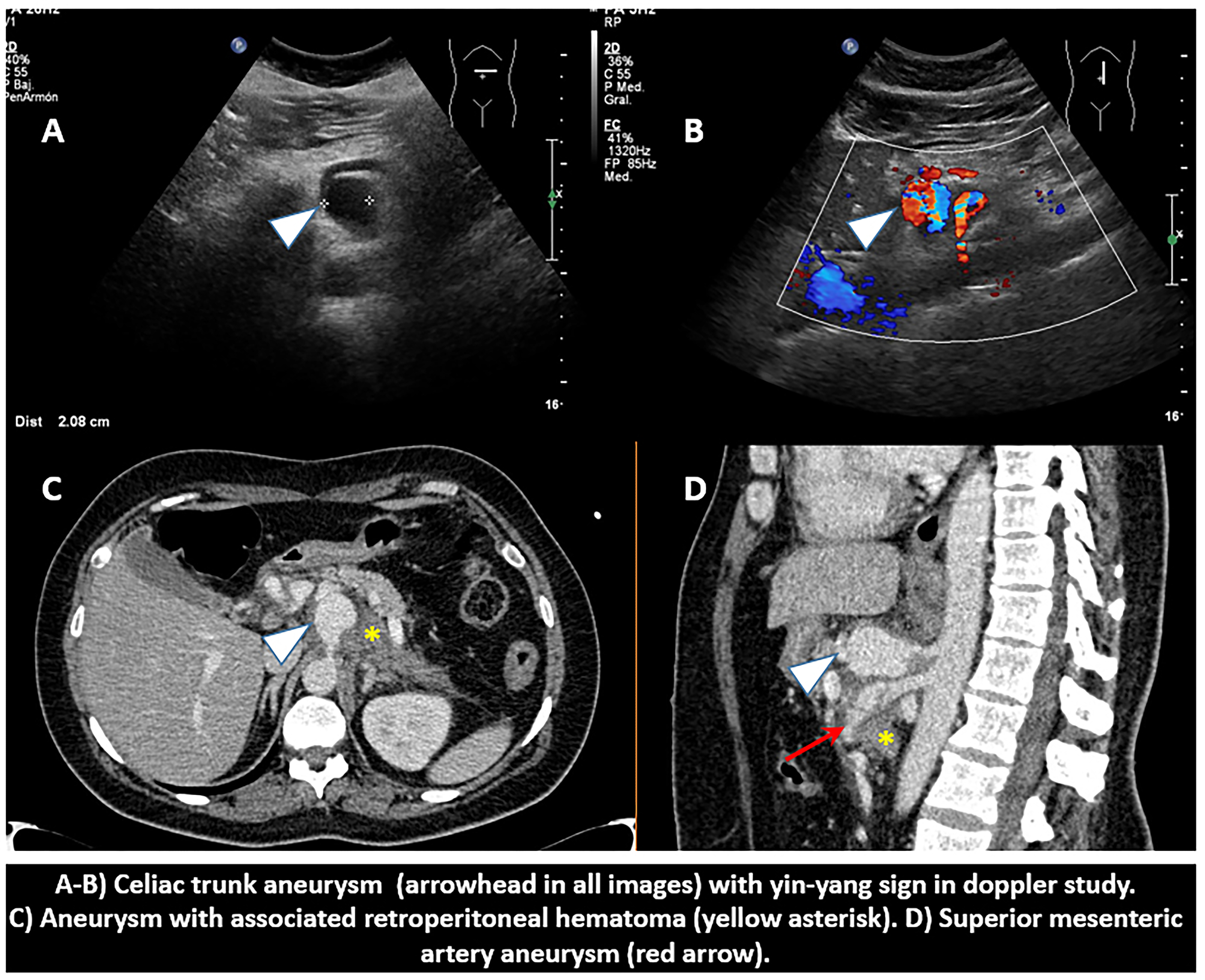
A 50-year-old woman with a medical history of neurofibromatosis type I, presents to our emergency department complaining of intermittent upper abdominal pain in the last 7 days, with associated nausea and vomiting. Abdominal examination reveals a soft abdomen with apparent tenderness to palpation in the epigastric and right upper quadrant region. Vital signs showed a blood pressure of 179/84 mmHg, a heart rate of 130 bpm and a temperature of 37.8°C. His laboratory values were as follows: - White blood cell count: 17,700 cells/µL - Hemoglobin level: 11.7 g/dL - Gamma glutamyltransferase level: 213 U/L - Alkaline phosphatase levels: 135 U/L With these findings we were asked to rule out a possible cholecystitis. On ultrasound, in epigastrium, we found a circumscribed anechoic saccular enlargement of celiac trunk with yin-yang sign at Doppler study. Findings where consistent with an aneurysm, however due to significant pain, we decided to perform a CT. Gallbladder had a normal appearance. Triphasic CT showed an aneurysm of 25 x 35 x 23 mm, which originated 11 mm from the outlet of the celiac trunk and had a neck of 4 mm. In addition, we also found an aneurysm of the mesenteric superior artery (MSA). As a variant of normality, the hepatic artery originated from de MSA. Around the aneurysms high density free fluid was identified, in relation to acute retroperitoneal hematoma. No signs of active bleeding were seen.
Discusión
Most frequent abdominal visceral aneurysms are splenic and hepatic aneurysms. They can be discovered incidentally or in the context of acute abdominal or multiple abdominal interventions. Its main complications are thrombosis, compression of adjacent structures and rupture. - Superior mesenteric artery aneurysms (5-7%): its natural history is progressive growth and subsequent rupture. Non-calcified aneurysms present a greater risk of breakdown. - Celiac trunk aneurysms (4%): they are usually diagnosed incidentally. As particular complications to be taken into account are those derived from hypoperfusion of the liver, spleen or stomach. The presence of a hematoma in the minor sac may be a sign of rupture of this type of aneurysm. Another important fact is that they are usually associated with other visceral aneurysms, so it is important to make a complete study.
Conclusión
A ruptured visceral aneurism may be a fatal condition, so early radiological diagnosis is essential. If there is one visceral aneurism, there may be another one.
Bibliografía
-Jesinger RA, Thoreson AA, Lamba R. Abdominal and Pelvic Aneurysms and Pseudoaneurysms: Imaging Review with Clinical, Radiologic, and Treatment Correlation. Radiographics 2013, 33:E71–E96. - McMullan DM, McBride M, Livesay JJ, Dougherty KG and Krajcer Z.