Hospital: Hospital Universitario Puerta de Hierro Majadahonda.
Nº: C2019-316
Aut@r o Autores: L. Gómez Pimpollo García, J. El-Khatib Núñez, J. Martínez González, J. San Miguel Espinosa, I. Hernández Delgado, M. Torres Navarro.
Presentación
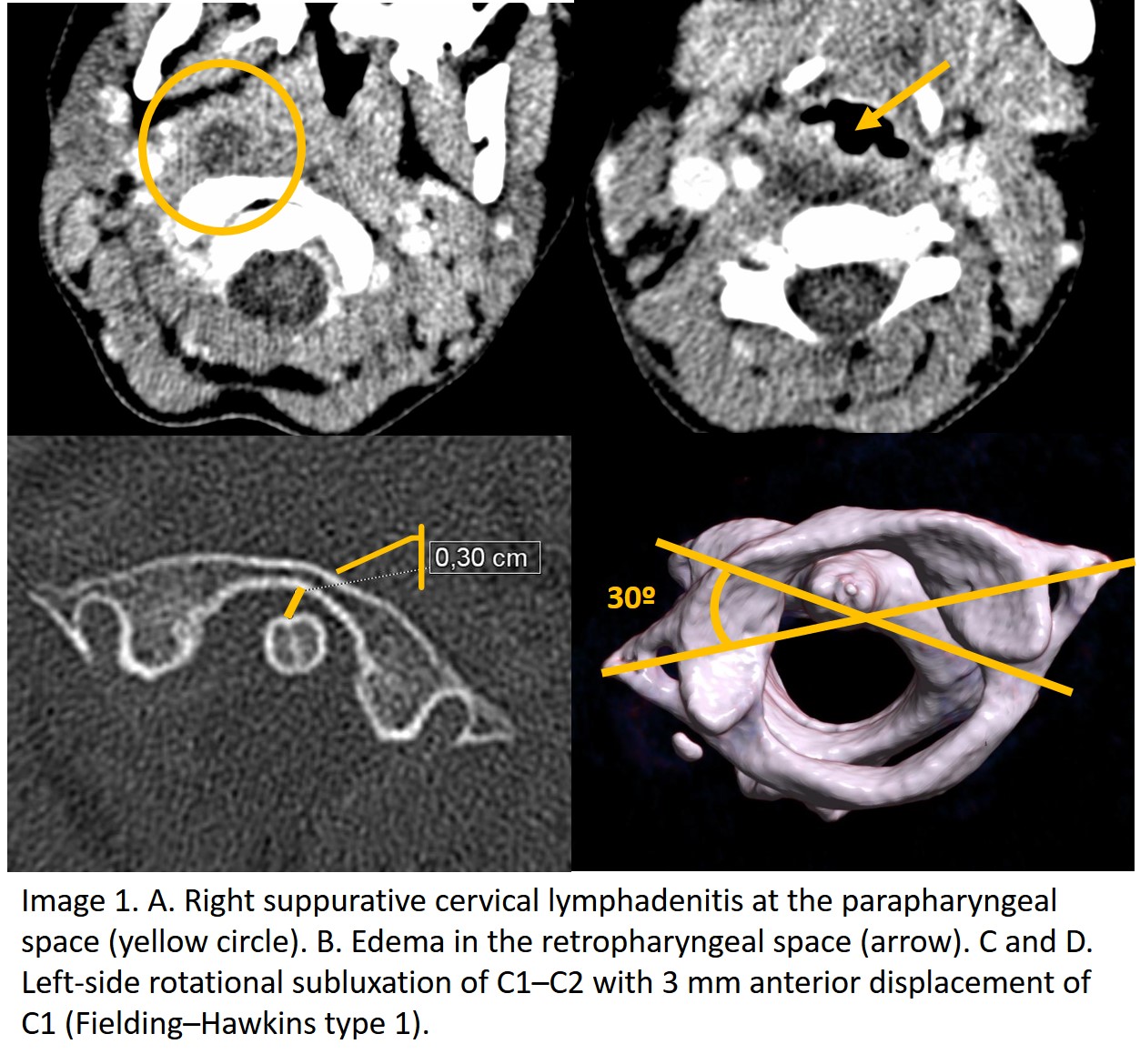
A 6-year-old girl referring neck pain last week and torticollis for 24 hours without history of trauma. Pharyngotonsillitis one week ago treated with amoxicillin-clavulanic acid for 4 days. Physical examination revealed hyperemic oropharynx without pillars bulging or uvula deviation, right cervical lymphadenopathies and limitation of cervical mobility, unable to reach neutral cervical position. Contrast-enhanced computed tomography (CT) at C1 level reveals right suppurative cervical lymphadenitis at the parapharyngeal space as a focal hypoattenuating, non-enhancing image, with associated edema in the retropharyngeal space. CT-scan also revealed left-sided rotational subluxation of C1–C2 with 3 mm anterior displacement of C1.
Discusión
Grisel’s syndrome is a non-traumatic subluxation of the atlantoaxial joint with intact atlantoaxial ligaments associated with infectious or inflammatory processes of the head and neck region, such as sinusitis, otomastoiditis, retropharyngeal abscess or an otolaryngologic (ORL) procedure (tonsillectomy, adenoidectomy, mastoidectomy, etc). The pathogenesis of Grisel syndrome is unclear, although it is presumed that hyperemia and abnormal relaxation of the occipito-atlantoaxial ligament complex result in atlantoaxial instability. It has almost exclusively been reported in children, due to major ligamentous laxity in children, however, adult cases may also occur. Classic presentation consists in a painful torticollis with previous upper respiratory tract infection or surgical procedure history. CT scan shows subluxation of the atlantoaxial joint and allows to classify it according to the degree of atlas displacement (Fielding– Hawkins classification): no displacement (type I), anterior displacement between 3 and 5 mm (type II), anterior displacement greater than 5 mm (type III) and posterior displacement (type IV). The first therapeutical step is intravenous antibiotherapy, oral anti-inflammatory and antispasmodic therapies. As the grade of subluxation increases, soft collar in type I, hard collar in type II, halo fixation in type III, and open fixation in type IV can be indicated. Surgery is indicated in case conservative treatment failure. Neurological complications, from radiculopathy to myelopathy and death by medullary compression can occur. Differential diagnosis should include muscular torticollis, abnormal ligament laxity (Down syndrome, connective tissue disorders), cervical spine instability or undetected trauma.
Conclusión
Grisel’s syndrome should be suspected in pediatric patient with painful torticollis and history of ORL infection or surgery. CT scan is the initial imaging test for diagnosis and classification. Early diagnosis and therapy are essential to prevent neurologic complications.
Bibliografía
- Haque S, Bilal Shafi BB, Kaleem M. Imaging of Torticollis in Children. RadioGraphics. 2012 Mar 1,32(2):557–71. - Pilge H, Prodinger PM, Bürklein D, Holzapfel BM, Lauen J. Nontraumatic Subluxation of the Atlanto-Axial Joint as Rare Form of Aquired Torti