Hospital: Hospital Universitario de Puerto Real.
Nº: C2019-439
Aut@r o Autores: A. Luna Morales, J. Pérez Herrera, E. Garcia, V. Lorenzo Quesada.
Presentación
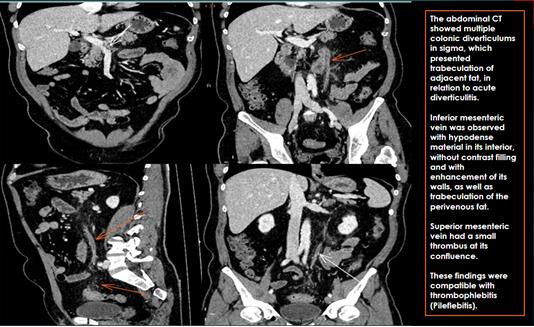
A 61-year-old man, hypertensive, with hypogastric abdominal pain and fever despite antibiotic treatment. In the blood tests, marked leukocytosis was observed with a predominance of polymorphonuclear cells and an elevated CRP. The abdominal CT showed multiple colonic diverticulums in sigma, which presented trabeculation of the adjacent fat, in relation to acute diverticulitis. Inferior mesenteric vein was observed with hypodense material in its interior, without contrast filling and with enhancement of its walls, as well as trabeculation of the perivenous fat. This vein drainded into the superior mesenteric vein, which had a small thrombus at its confluence. These findings were compatible with thrombophlebitis (Pileflebitis). The patient was treated with anticoagulants and antibiotics, with favorable evolution.
Discusión
Pylephlebitis is the acutely septic thrombophlebitis of the portal vein and / or its branches, and it’s usually a complication of intra-abdominal inflammatory processes or surgical interventions in patients with blood dyscrasias. Its diagnosis is late and as etiology are included appendicitis, complicated diverticulitis, inflammatory bowel disease, acute pancreatitis, cholangitis and acute cholecystitis. In the antibiotic era, the most frequent cause is colonic diverticulitis, surpassing appendicitis. It is a very low frequency entity due to the early use of antibiotics, but it is relevant due to its high mortality rate (20-30% in some series). The infectious process extends through peripheral mesenteric branches, alters the vascular endothelium and causes the appearance of thrombosis, it tends to spread, affecting at the end the portal vein and its intrahepatic branches, which can cause liver abscesses. The germs involved are Gram negative (E. coli) and aerobic streptococci, and sometimes anaerobes such as Bacteoides fragilis. The clinic is nonspecific, with fever, chills, nausea, vomiting, nonspecific abdominal pain and often jaundice. The diagnosis is established by CT scan, by identifying the intraabdominal inflammatory process and the presence of a hypodense central area in the portal vein and / or its tributaries, accompanied by wall enhancement and infiltration of perivenous fat. The treatment consists on broad-spectrum antibiotic therapy for the risk of liver abscess formation, Controversy exists regarding the use of anticoagulation.
Conclusión
The knowledge and early diagnosis of pylephlebitis as a remote complication of abdominal infectious / inflammatory processes is fundamental for an adequate management of these patients that has an impact on their evolution, given their high mortality.
Bibliografía
- Lee H, Park S, Yi B, Yeon E, Kim J, Hong H. Portal vein thrombosis: CT features. Abdominal Imaging. 2007,33(1):72-79. - Bartone G, Severino B, Armellino M, Domenico Maglio M, Castriconi M. Clinical Symptoms of Intestinal Vascular Disorders. Radiologic