Hospital: Madrid Puerta del Sur.
Nº: C2019-250
Aut@r o Autores: V. Navarro, D. Camacho, L. Arrieta, L. Figueroa, M. Javier, V. Pérez. Hospitales
Presentación
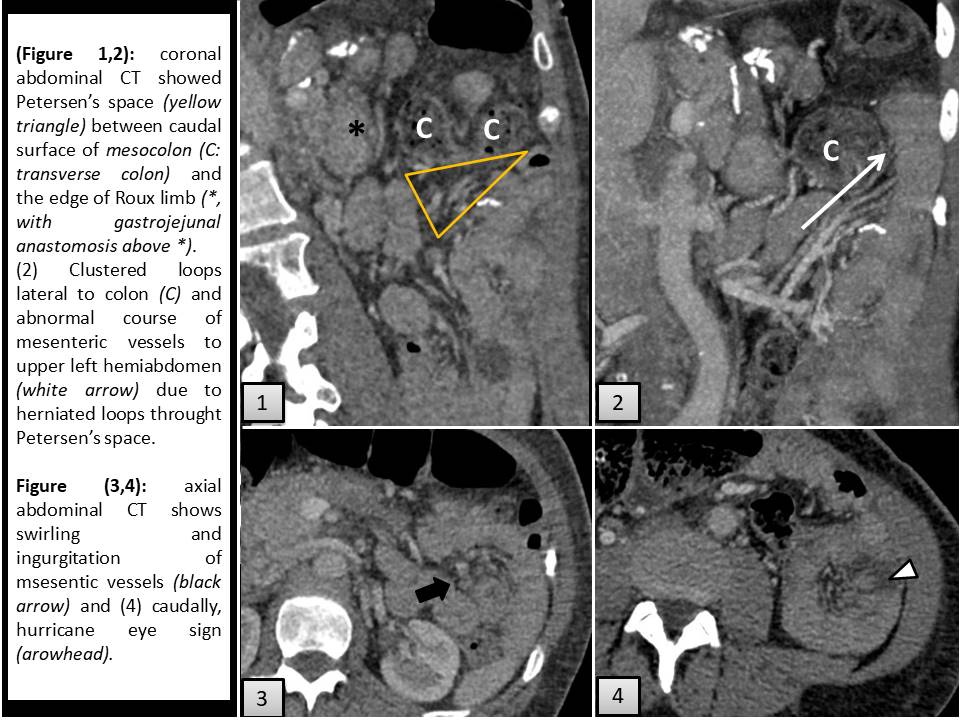
A 46-year-old woman with laparoscopic Roux- en – Y gastric bypass procedure (RYGBP) performed a year ago was admitted to emergency department due to vomiting, colic abdominal pain and fever over last two days.Abdominal examination revealed distention and moderated tenderness. Laboratory findings were normal. Abdominal enhanced CT was performed in portal phase. It showed a cluster of small bowell in upper left hemiabdomen, lateral to colon, with torsion and swelling of its mesentery, as typical indirect signs of internal hernia (IH). According to the location, Petersen’s hernia(PH) was suggested.
Discusión
Exploratory laparotomy found small bowell obstruction (SBO) and mesenteric ingurgitation secundary to IH throughout Petersen space. There were no ischemic signs neither further complications in postoperative course.Obesity and bariatric surgery has grown together due to fail to lose weight with nonsurgical treatments. RYGBP has the highest long term success rate (1).Loss of mesenteric fat after RYGBP wides intermesenteric spaces. Laparoscopic procedure and no primary closure of them are associated with higher incidence of IH. One of the spaces is Petersen’s, which is located between the caudal surface of mesocolon and the edge of Roux limb(2). Their symptoms are unspecific, presented as intermitent herniation or acute incarceration and threatened SBO. CT scan is the gold standard for IH. Lack of knowledge of RYGBP may lead incorrect diagnosis. Most of CT may be reported as normal either with minor obstruction or absence of direct signs (1,2) as our case.Diagnosis could be made by combination of 7 signs(2) with variable sensitivity(S) and especificity(E): - SBO and swirling of mesentery were the best accurated signs(S=96%, E=87%). In our case, the abnormal distribution and swirling of mesenteric vessels increased our suspicion. - SMV beaking and SBO signs provides the highest specificity (S=90%, E=92%). - As single sign, the reversed orientation between superior mesenteric artery (SMA) and superior mesenteric vein (SMV) has the highest sensitivity. However, it may happen in normal condition so it must be rewied carefully. - Clustered loops, mushroom shaped bowells, bowel other than duodenum behind SMA and right-sided location of jejunojejunostomy were more specific but far less sensitive. Distal mesenteric fat surrounded by herniated bowel loops show hurricane eye sign, detected in our case.
Conclusión
Radiologists must be aware of potential IH after RYGBP. Mostly of cases are diagnosed by using indirect signs without SBO.
Bibliografía
- Carucci L, Turner M, Shaylor S. Internal henial following Roux – en – Y bypass gastric surgery for morbid obesity: evaluation of radiographic findings at small bowell examination. Radiology 2009,251:762-770. - DIlauro M, McInnes M, Schieda N. Internal