Hospital: Northwick Park hospital.
Nº: C2019-755
Aut@r o Autores: N. Tyagi, H. Hirji, M. Arora, P. Karia, H. Taufik, S. Desigan.
Presentación
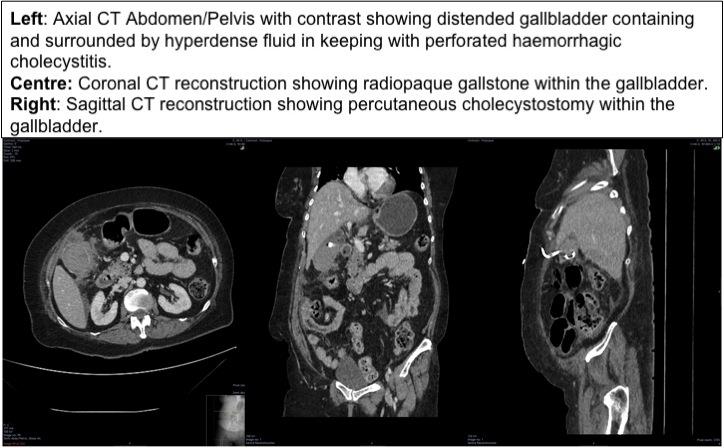
A 70 year old female with a background of Schizophrenia and Type 2 Diabetes but usually fit and independent, presented with a days history of right sided abdominal pain. She was peritonitic on clinical examination with tachycardia. Blood tests showed elevated inflammatory markers (CRP 310, WCC 25.3x10^9), slightly raised ALP and bilirubin. Her haemoglobin initially was 110 g/L, but fell to 83 g/L. She was reviewed by the surgical team and a CT scan was performed. The CT scan showed a distended gallbladder containing and surrounded by hyperdense fluid (HU 50-60) with associated fat stranding. A 6mm radiopaque gallstone noted within this. These findings were suspicious for a perforated haemorrhagic cholecystitis (see image). The patient had an emergency US guided cholecystostomy which showed a thick walled gallbladder containing and surrounded by echogenic material and ascites. Haemorrhagic bile was aspirated and confirmed the CT diagnosis.
Discusión
A perforated haemorrhagic cholecystitis is a rare complication of acute cholecystitis with a high morbidity/mortality, with few reported cases1-2. The exact pathophysiology is unknown but the theory suggests ischaemic erosion of the gallbladder wall by transmural inflammation. There are some conditions which may predispose to this such as renal failure, haemophilia, vasculitis, anticoagulants and trauma although none were identified in this patient. Given the similarity in clinical presentation with acute cholecystitis but with an increased associated morbidity and mortality, early cross sectional imaging is vital in establishing this diagnosis.2-3 Demonstration of high density fluid within the gallbladder should be seen as suspicious for haemorrhage. When this fluid extends beyond thegallbladder wall, it is concerning for perforation even if no definite wall defect is identified. There are no clear guidelines on the management of these patients due to the rarity of this finding. Treatment is dictated by their clinical status and co-morbidities.4 This may include cholecystectomy, cholecystostomy, or conservative management with antibiotics alone. In this particular patient an ultrasound guided cholecystostomy was performed providing symptomatic relief. Subsequently over the course of a few days, the inflammatory markers also improved.
Conclusión
A perforated haemorrhagic cholecysitis is a rare and severe consequence of acute cholecystitis with a high morbitidy and mortality. There are very few cases in the literature with regards to imaging findings and management.
Bibliografía
- Tarazi M, Tomalieh FT, Sweeney A, Sumner D, Abdulaal Y. Literature review and case series of haemorrhagic cholecystitis. J Surg Case Rep. 2019, 1: 1-4 - Aljiffry MM, Almulhim AN, Jamal MH, Hassanain MM. Acute cholecystitis presenting with massive int