Hospital: HCUVA
Nº: C2019-327
Aut@r o Autores: G. De Paco Tudela, G. Litrán López, A. Castillo García, A. Cuélliga González, V. Orcajada Zamora, D. Gea Martos.
Presentación
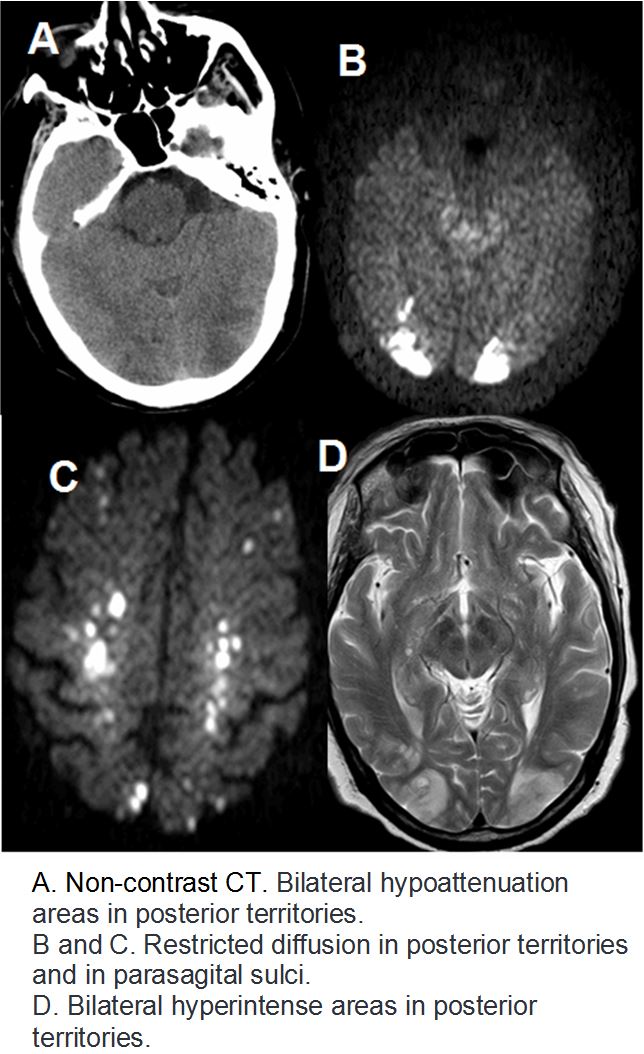
A 60-year-old man with a medical history for lung adenocarcinoma IIIB under treatment with nivolumab, presented to emergency of our hospital due to confusion, weakness in right upper limb as well as bilateral visual blur. The patient's Glasgow Coma Scale score was 11, and his temperature was normal. Non-contrast CT was performed, and the findings were occipital bilateral hypoattenuation areas (Figure A), as well as nodular hypodense cortical lesions at parasagital frontal sulci. Two days later a brain RM was performed, showing symmetrical bilateral corticosubcortical occipitoparietal hyperintense T2 lesions as well as at precentral sulci (Figure D).These areas presented diffusion restriction (Figures B and C) with signal fall in ADC maps. No leptomeningeal o nodular enhacement was evidenced. These findings were compatible with posterior symmetrical and bilateral cytotoxic/vasogenic edema, suggestive of posterior reversible encephalopathy syndrome with acute-subacute stroke and hemorragic transformation. Nivolumab treatment was suspended and corticosteroids were administered but, due to the established ischaemic lesions, visual loss remained without any changes.
Discusión
PRES's aetiology is thought to be related to the dysfunction of the endothelium of the bloodbrain-barrier. The diagnostic should be considered in the setting of acute neurological symptoms in patients with blood pressure fluctuations, use of cytotoxic drugs, autoimmune disorders, or eclampsia. The rapid withdrawal of the trigger is the first action to be taken to avoid complications. Corticosteroids and antihyperthensive drugs can be administered in order to reduce vasogenic edema and reduce blood pressure, respectively.
Conclusión
There is a large amount of references that link conventional chemotherapy and PRES, but just a few of nivolumab-induced PRES, and due to it is an increasingly used antitumoral drug, this diagnosis should be taken in consideration in cancer patients presenting with acute mental status changes after recent immune therapy.
Bibliografía
- Hussein HM, Dornfeld B, Schneider DJ. Nivolumab-induced posterior reversible encephalopathy syndrome. Neurol Clin Pract. 2017,7(5):455-456. - McKinney AM, Short J, Truwit CL, McKinney ZJ, Kozak OS, SantaCruz KS, et al. Posterior reversible encephalopat