Hospital: Complejo Hospitalario de Navarra.
Nº: C2019-610
Aut@r o Autores: L.A. De Llano Ibisate, P. Lopez Sala, N. Alonso Ordás, N. Alberdi Aldasoro, G. Unzue Garcia-Falces, T. Lage Vidal.
Presentación
A 43-year-old man with no history of interest or cardiovascular risk factors, came to the ER because after exercising (doing weights and running) he began to feel periocular and frontal headache with decreased visual acuity. It lasted about an hour and then improved. When the neurologists explored him they observed that he had not a totally fluid language, with some paraphasia, although the headache has improved. Their suspected diagnosis was a fluctuating neurological focus (migraine with prolonged aura vs AIT), so we perform a CT with stroke protocol.
Discusión
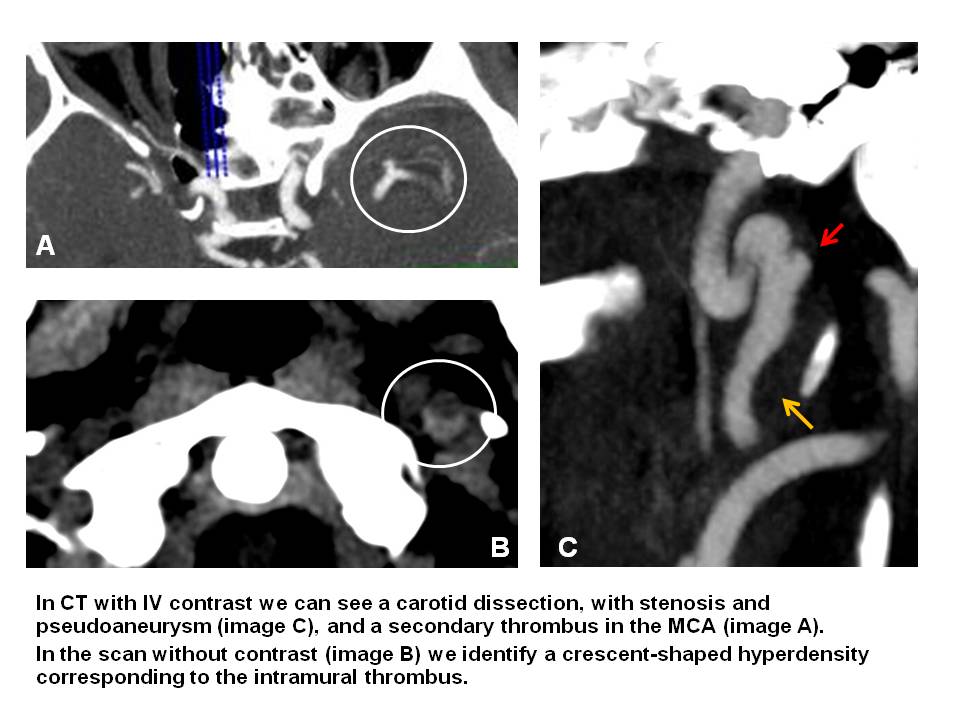
In CT without contrast, no early signs of ischemia or bleeding were seen. In CT perfusion maps a significant area of penumbra in the territory of the left MCA was seen and in the CT angiography study we could see an occlusion in the M1 segment of the left MCA. It seemed that the case was already resolved, but we should never forget to review the entire study. Carotid dissection is responsible for more than 25% of brain strokes in young and middle-aged adults, and headache is the most frequent symptom. In a young person without cardiovascular risk factors, especially after doing exercise, we should suspect the possibility of a carotid dissection and look the study very carefully. The extracranial segments of the carotid artery are more likely to dissection, due to the greater mobility in this region and the greater probability of being damaged by contact with bony structures (styloid process and cervical spine). In the CT without contrast we can see a crescent-shaped hyperdensity that corresponds to an area of intramural hematoma, which compresses the true lumen, causing a stenosis of the arterial lumen. If the dissection extends to the adventitia a pseudoaneurysm may form, which may cause distal thromboembolic events. In our case, the patient had a carotid dissection (difficult to see if you do not look for it) that caused a distal thrombus in the MCA (Image 1).
Conclusión
We must always make a joint diagnosis between clinicians and radiologists, and more in a stroke code, where the suspected diagnosis can be very helpful for us, because as we all know, you can not find what you are not looking for. Besides, we should never forget to review the entire study. In our case, the patient had a thrombus in the MCA secondary to a dissection in the internal carotid.
Bibliografía
- M. Diez, E. Lopez, M. Drake, S. Sánchez, J. M. Navasa, E. M. Marco. Cómo detectar las disecciones carotídeas en la TC del código ictus. Guía de la superviviencia para la guardia. SERAM 2014 - A. M. Staitie, P. Puyalto