Hospital: Hospital de 12 Octubre.
Nº: C2019-620
Aut@r o Autores: P. Encinas, I. Navas, R. Castro, G. Galarraga, M. De La Puente, L. Ibáñez.
Presentación
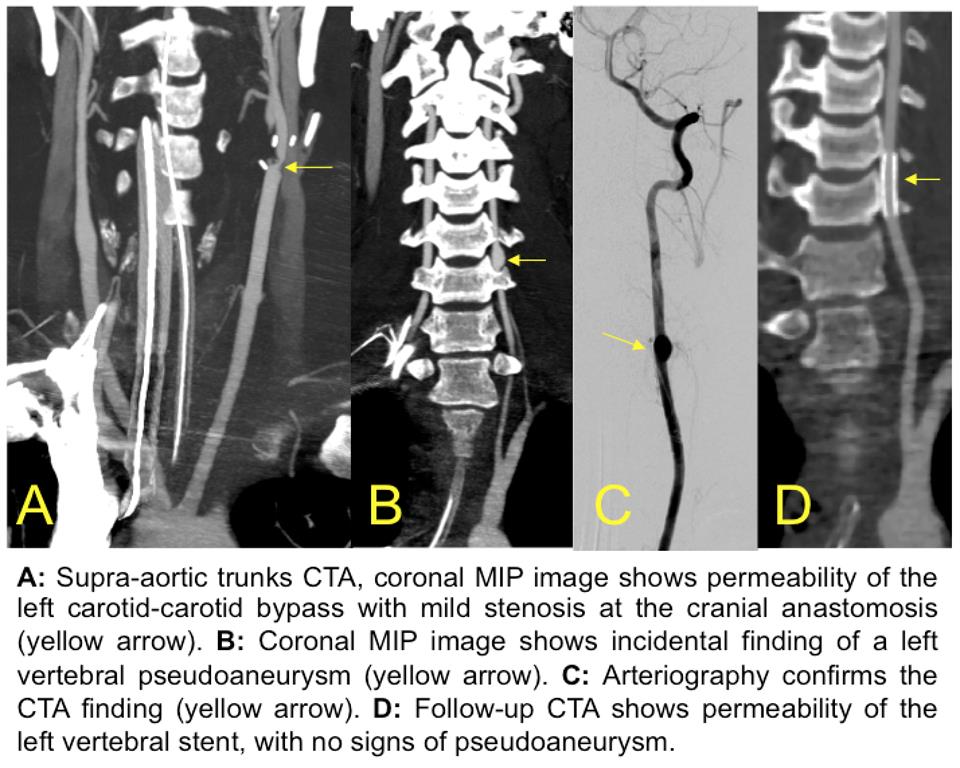
A 17 years-old male is admitted to our hospital due to a neck stab wound. Upon arrival the patient is unconscious and hemodynamically unstable. Physical exploration demonstrates a left penetrating laterocervical injury with signs of active arterial bleeding. He is rushed to the operating room, finding a left common carotid section, a carotid-carotid bypass is performed with good results, achieving hemodynamic stability. Immediate post-operatory computed-tomography angiography (CTA) shows permeability of the left carotid-carotid bypass with no signs of contrast extravasation, although mild stenosis (50%) at the site of anastomosis is noted. Incidentally, a left vertebral pseudoaneurysm is seen at the level of C5-C6 (V2 segment). An arteriography confirms the CTA findings and an endovascular stent is placed with excellent morphologic results. Follow-up CTA shows no complications.
Discusión
Penetrating neck trauma remains a challenging condition, as it demands a clear anatomical knowledge for a proper diagnosis and management. The existence of vital structures confined in a small area like the neck are strongly related with a diversity of injuries that demand urgent attention, such as aerodigestive, vascular and cervical spine injuries. Anatomically the neck is divided in three zones (I: lower neck, II: midneck, III: upper neck), of which zone II (between the cricoid cartilage and the angle of the mandible) is the most commonly injured (2). The zone of injury refers to the site of entry wound and the wound track may cross neck zones, as well as the face, cranium or thorax (3). Higher mortality rates are seen in zone I injuries (below the cricoid cartilage) due to the proximity of mediastinal structures, severity of vascular injuries and surgical challenges (may require both transcervical and transthoracic approaches). Approximately 15%–25% of penetrating injuries to the neck result in an arterial injury (4). Exsanguination is the most common cause of death and the carotid artery is the structure most commonly involved. Arterial injuries have worse outcomes as they often present with neurological events such as stroke. Besides a careful physical exploration, CT angiography is a fast, safe, and reliable noninvasive method for evaluating patients with penetrating neck trauma.
Conclusión
Physical and even surgical exploration may not be enough in neck penetrating injuries. Imaging studies, especially CTA, provide quick and vital information for a correct multidisciplinary management.
Bibliografía
- McConnell DB, Trunkey DD. Management of penetrating trauma to the neck. Adv Surg. 1994,27:97 - Scott D. Steenburg S, Sliker C, Shanmuganathan K, Siegel E. Imaging Evaluation of Penetrating Neck Injuries. RadioGraphics 2010 30:4, 869-886 - Nú&