Hospital: Ramon y Cajal University Hospital.
Nº: C2019-522
Aut@r o Autores: M. Vicente-Redondo, C. Suevos-Ballesteros, L. Alonso De Caso García, B. LumbrerasFernández, F. González-Tello, N. Almeida-Arostegui.
Presentación
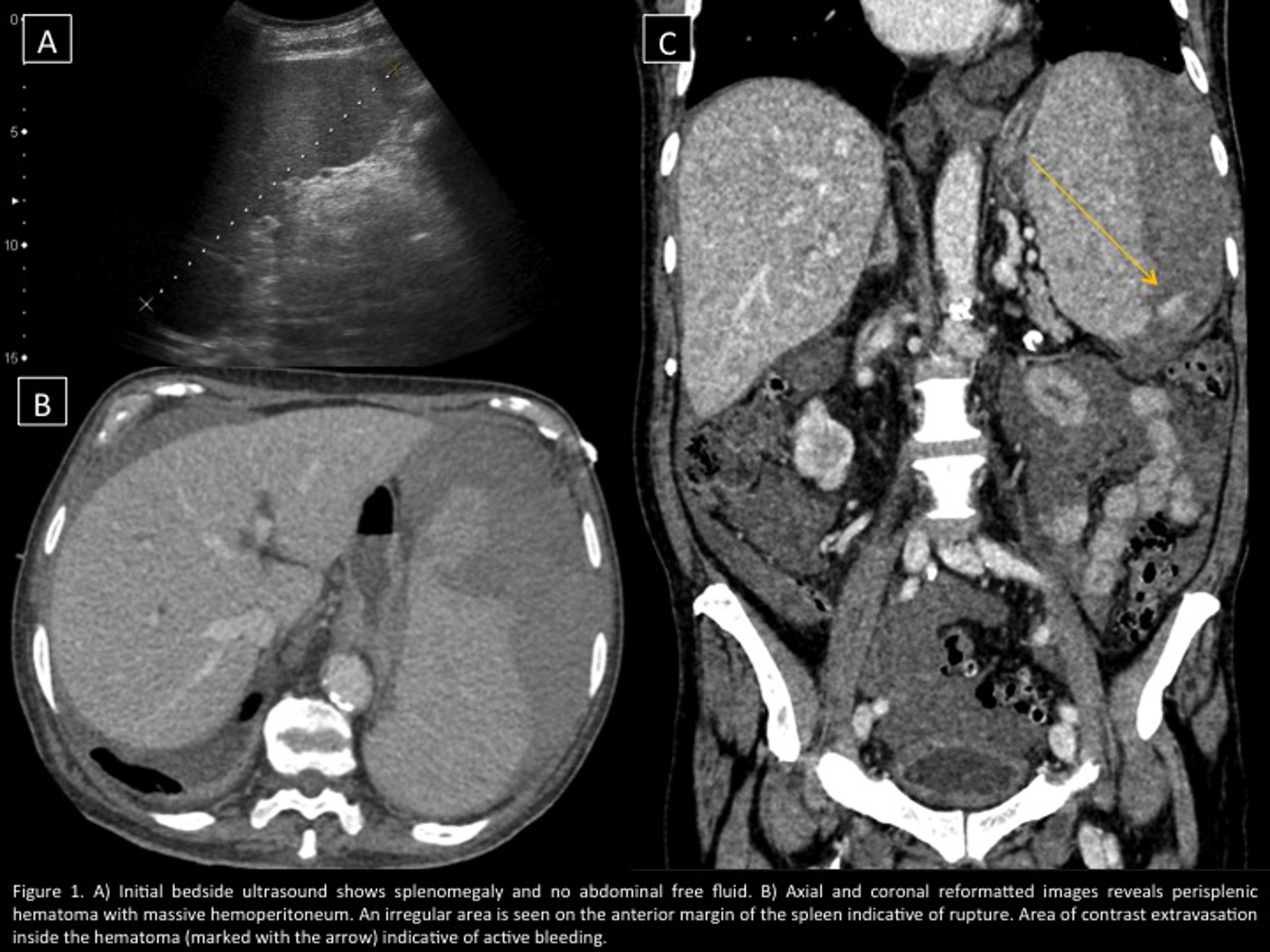
An 82-year-old man presented to the emergency department with sudden-onset leftsided abdominal pain and increasing abdominal distention. The pain worsened with movements and Valsalva and did not subside after taking NSAIDs. On initial examination his pulse was 77 bpm and BP 130/55 mmHg. Chest examination was unremarkable. Abdominal examination showed left-sided tenderness. A bedside ultrasound was performed (Figure 1, A), which showed marked enlarged spleen without any other finding of interest. The patient spent the night under observation and a few hours later his BP suddenly dropped to 80/50 mmHg and his pulse increased to 120 bpm. Following initial successful fluid resuscitation he underwent abdominal computerized tomography (CT)(Figure 1, B-C). Contrast-enhanced CT revealed a large perisplenic hematoma in the left upper quadrant with massive hemoperitoneum. An irregular hypodense area was identified on the anterior margin of the splenic superior pole. In addition, there was an area of contrast agent extravasation in the arterial phase which increased in amount and density in the venous phase.
Discusión
On the basis of computed tomography findings, diagnosis of splenic rupture with signs of active bleeding was made. Patient was immediately taken up for surgery. Intraoperative findings showed enlarged spleen with large intra and perisplenic haematoma. Significant hemoperitoneum was there. Splenectomy with complete haemostasis was done. In most cases splenic rupture is due to trauma. However, our patient denied any history of trauma. This disease is often not considered in the differential diagnosis of abdominal pain in the left hypochondrium in the absence of trauma, which ranges from pathology in the pancreatic tail to renal causes. Nevertheless, the remarkable fact about the case was the lack of a cause to explain the rupture. The causes of splenic atraumatic rupture are varied and include infectious,hematological, inflammatory, iatrogenic, splenic causes or idiopathic. We did a research in the patient’s medical history and as significant finding, the patient had been diagnosed with polycythemia vera and was under treatment with hydroxycarbamide. Spontaneous rupture of the spleen is occasionally seen in the hematological malignancies. It has been reported that male sex, adulthood, splenomegaly and chemotherapy are factors that are associated with it and our patient met all risk factors.
Conclusión
To conclude, spontaneous splenic rupture is a rare complication of haematological malignancies. The diagnosis should be considered in a patient who presents with left upper quadrant pain, hypotension and tachycardia. Ultrasound and CT are the diagnostic modalities of choice. Aggressive management with early surgical intervention and appropriate hemoderivative support is crucial.
Bibliografía
- Gedik E, Girgin S, Aldemir M, Keles C, Tuncer MC, Aktas A. Non-traumatic splenic rupture: report of seven cases and review of the literature. World J Gastroenterol. 2008,14(43):6711-6.