Hospital: Hospital Universitario de 12 Octubre.
Nº: C2019-519
Aut@r o Autores: C. Fernández Cabrera, I. Navas Fernández-Silgado, M. Depetris, C. Cruz Conde, E. Martínez Chamorro, S. Borruel Nacenta..
Presentación
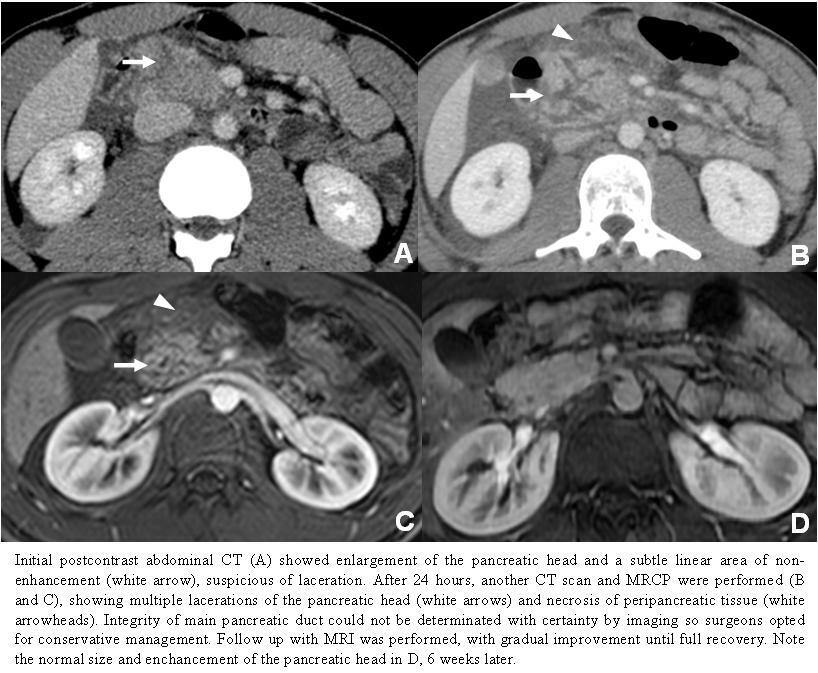
A 17 year-old boy presented to the emergency room with epigastric pain and vomiting after a football game. Physical examination of the abdomen showed an epigastric bruise, where the patient suffered a direct blow from an opponent’s knee during the game. Serum amylase was 404 U/L. Serial computed tomography (CT) scans with intravenous contrast were performed and revealed traumatic pancreatitis and large pancreatic head lacerations with no associated vascular injury. The patient was managed conservatively and followed up by serial magnetic resonance imaging (MRI) which revealed gradual improvement until full recovery 6 weeks later.
Discusión
Blunt abdominal trauma is the major cause of abdominal injury in children. Pancreatic injury is uncommon, but its fixed position anterior to the vertebral column makes the organ vulnerable to compression injuries. This was the case with our patient, in whom the pancreatic head was compressed between an opposing player's knee and his spine. Most blunt pancreatic injuries occur in the pancreatic body. Those to the pancreatic tail and head are less common. When a pancreatic injury occurs, serum amylase may raise but laboratory findings do not indicate the severity of the injury. CT is used as screening for patients with abdominal trauma and is considered the most effective modality for diagnosing pancreatic injury, although initial CT findings of patients with pancreatic injuries may be within normal limits in the first 12 hours after the injury. But CT is limited in detection pancreatic duct injury, which is determinant for surgical intervention. In fact, disruption of the pancreatic duct is generally treated surgically, whereas injuries without duct involvement are usually treated with drainage and observation. MRCP or endoscopic retrograde cholangiopancreatography (ERCP) should be also performed. Pancreatic lacerations are seen as poorly enhancing linear lesions, often perpendicular to the long axis of the pancreas, associated to swelling of the involved pancreatic segment, acute peripancreatic fluid collections and free fluid. Some pancreatic injury grading systems have been proposed in order to standardize CT diagnoses and to allow objective management. Major variables are anatomic site, the type of injury (hematoma, laceration or transection) and the state of the pancreatic duct. The most accepted system today was published by the American Association for the Surgery of Trauma (AAST) and differentiates between grades I to V.
Conclusión
Isolated pancreatic injury although uncommon can occur and requires close attention to the subtle signs of injury. In our case, despite the extensive pancreatic lacerations, the patient’s outcome was successful without surgery.
Bibliografía
- Linsenmaier U, Wirth S, Reiser M, and Körner M. Diagnosis and Classification of Pancreatic and Duodenal Injuries in Emergency Radiology. RadioGraphics 2008 28:6, 1591-1602.