Hospital: Hospital Universitario Ramon y Cajal.
Nº: C2019-531
Aut@r o Autores: A. Olavarria Delgado, I. Pecharroman De Las Heras, R. Romera Sanchez, A. Palomera Rico, I. Garcia Gomez Muriel, C. Picon Serrano.
Presentación
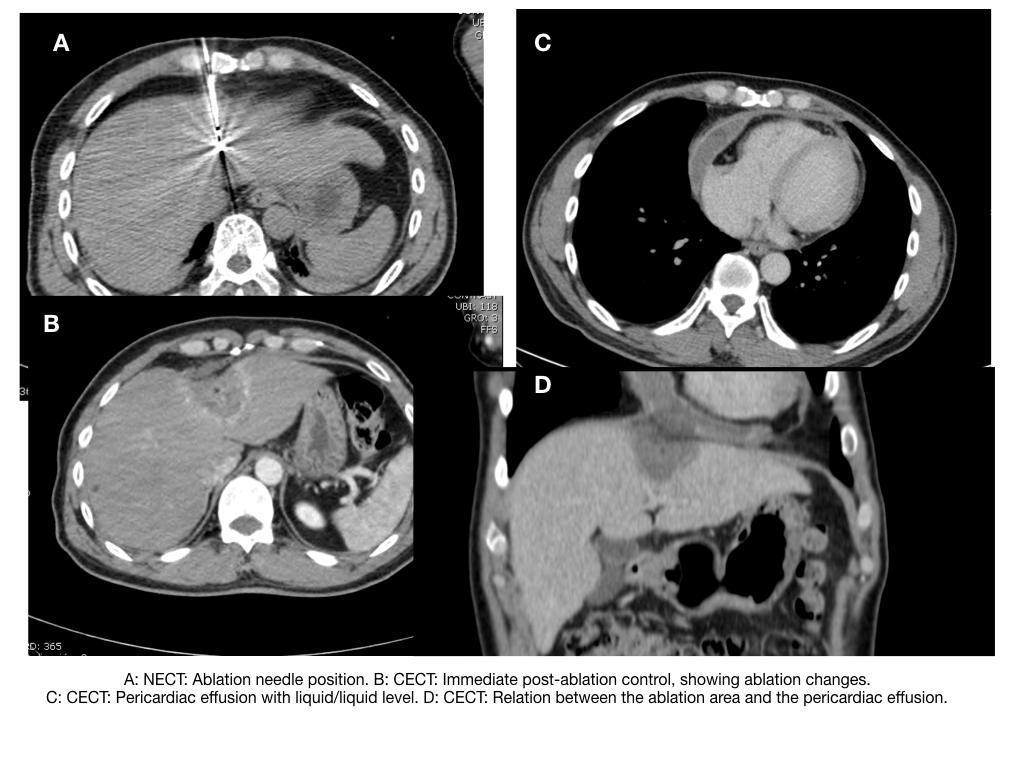
44 years old male patient. Consults to the ER for epigastric and mid-chest noncontinuous pain, that worsens with coughing, breathing and position changes. Symptoms started after MW ablation of liver lesion 3 weeks earlier. No fever. Prior history of HBV cirrosis, with 24 mm HCC in segment II. PE: BP:106/81 mmHg, HR: 96 bpm O2Sat: 100% Tº 35,7ºC. No exertion of pain on thorax or abdomen on examination. Lab test: elevated C-reactive protein and platelets. Normal cardiac enzymes. EKG: Negative T wave in anterior-inferior segment. Echocardiogram(Echo): Hipoechoic lesion located to the right of the tricuspid valve, regarded as extra-cardiac. Normal RV and LV, no mass effect or other significant findings.
Discusión
Although, Echo is the imaging technique of choice for evaluation of pericardial effusion and cardiac tamponade, CT has the advantage of evaluating the suspected pericardial disease and the adjacent structures. CT allows the measurement of attenuation values of the collection. Pericardial fluid with attenuation values close to that of water is likely to represents a simple serous effusion, while higher attenuation values suggest hemopericardium, malignancy, purulent exudates, or myxedematous effusion. CT also allows the identifcation of nodular areas within the pericardial thickening, the typical anterior location of the thickened pericardium orlack of change at decubitus positioning. In the presented case, the clue lies in the history of thermal ablation of a lesion located in the left lobe domus, near the chest cavity. The relatively mild symptoms, the absence of cardiac tamponade and the identification of an “extra pericardiac” lesion on Echo, probably correlates to the method of injury, originated at a distance from the heart. Pleural effusion was probably reactive in nature, with an accompany hematoma outside the pericardium. In thermal ablation is of paramount importance to identify the posible sites of complication, since changes in patient position and/or hidrodissection can avoid this kind of complications. In those cases in which the risk can be minimized but not completely avoided the patient should be informed on both the risks and treatment alternatives. Post-procedure surveillance should be maximized.
Conclusión
Pericardium evaluation is mostly done with echocardiogram, for the reasons of accessibility, absence of radiation, and capability of assessing the pericardium and heart function. Although, in certain situations the wider field of examination provided by CT can offer the clues to a better evaluation. Extra abdominal complications of thermal ablation in the liver are rare but simple to explain with certain knowledge of the technique and awareness on the location of the ablated lesion.
Bibliografía
- Rhim H, Yoon K-H, Lee JM, Cho Y, Cho J-S, Kim SH, et al. Major Complications after Radio-frequency Thermal Ablation of Hepatic Tumors: Spectrum of Imaging Findings. RadioGraphics, 2003 Vol.23, No.1:123-134 - Restrepo CS, Lemos DF, Lemos JA, Velazquez E