Hospital: Osakidetza HU Cruces.
Nº: C2019-643
Aut@r o Autores: B. Souto Canteli, S. Laburbu Zabala, L. Prada San Martín, A. Coll I Prat, J. Mendiola Arza, A. Dolado Llorente.
Presentación
We report a case of a dural arteriovenopus fistula (DAVF) which debuted as an intraparenquimatous hematoma. Patient came to Emergency Department with clinic of pulsatile cephalea, progressive left sensitive deficit, dizziness and instability. CT protocol for acute stroke was performed: computed tomography (CT), perffusion CT and CT angiography.
Discusión
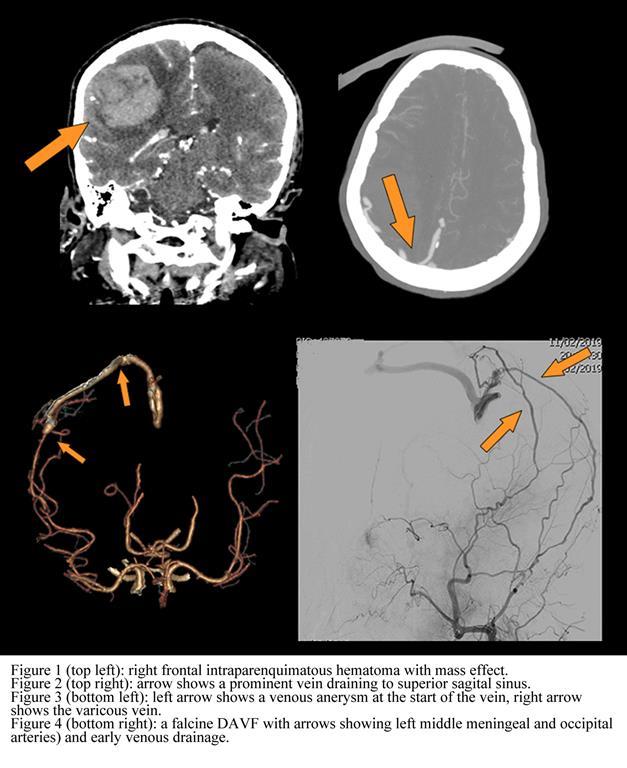
CT showed a right frontal intraparenquimatous hematoma with mass effect on the right cerebral hemisphere and results in leftward midline shift and subfalcine and right uncal herniations. CT angiography showed a prominent, varicous, venous cortical drainage to superior sagital sinus from the intraparenquimatous hematoma. Also, at the start of the venous drainage, a venous aneurysm was detected. Dural arteriovenous fistula (DAVF) was suggested as the most probable diagnosis because of this enlarged vein, and the abscense of other features that may indicate an alternative diagnosis, such as a nidus (arteriovenous malformation) or enlarged pial arteries (pial arteriovenous fistula). Digital subtraction angiography (DSA) revealed that many arterial branches feed the DAVF: left middle meningeal (main apport) and occipital arteries and right superficial temporal, tentorial and calcarine arteries. Diagnosis was a falcine DAVF Cognard grade IV. Interventional radiologists embolized the outfall of the venous drainage, excluding the DAVF.On follow up, patient had no complications with complete resorption of the hematoma.DAVF are abnormal communications within the dural leaflets, between meningeal arteries and dural venous sinuses and/or subarachnoid veins.Its incidence is calculated for 10-15% of all intracranial vascular malformations. Although DSA remains the gold standard for detecting and evaluating a suspected DAVF, it is important to suspect it in non invasive imaging techniques when some features are observed: intracranial hemorrhage, hydrocephalus, cerebral edema related to venous congestion, venous sinus occlusion or enlarged cortical veins. Key features in DSA are the presence of early venous drainage due to an abnormal communication within the dural arterial system and dural venous sinuses and/or subarachnoid veins. This feature is the base of current clasiffication systems: Cognard and Borden. The higher the grade the higher probability of a more agressive debut and the worse the natural history, including hemorrhage (as on our case) or neurological deficits.
Conclusión
It is important to suspect a DAVF in non invasive imaging techniques when some features are observed: intracranial hemorrhage, hydrocephalus, cerebral edema related to venous congestion, venous sinus occlusion or enlarged cortical veins.
Bibliografía
- Sasikhan G, Sirintara P, Pakorn J, Manohar MS, Derek CA, Timo K, et al. Radiologic assessment of brain arteriovenous malformations: what clinicians need to know. RadioGraphics 2010,30(2):483–501. - Chung-Wei L, Adam H, Yao-Hung W, Chung-Yi Y, Ya-Fang C