Hospital: Hospital Ramón y Cajal.
Nº: C2019-154
Aut@r o Autores: J. Montilla López-Gay, N. Almeida Arostegui, C. Campos Ferrer, B. Lumbreras, I. Pecharroman, P. Marazuela García.
Presentación
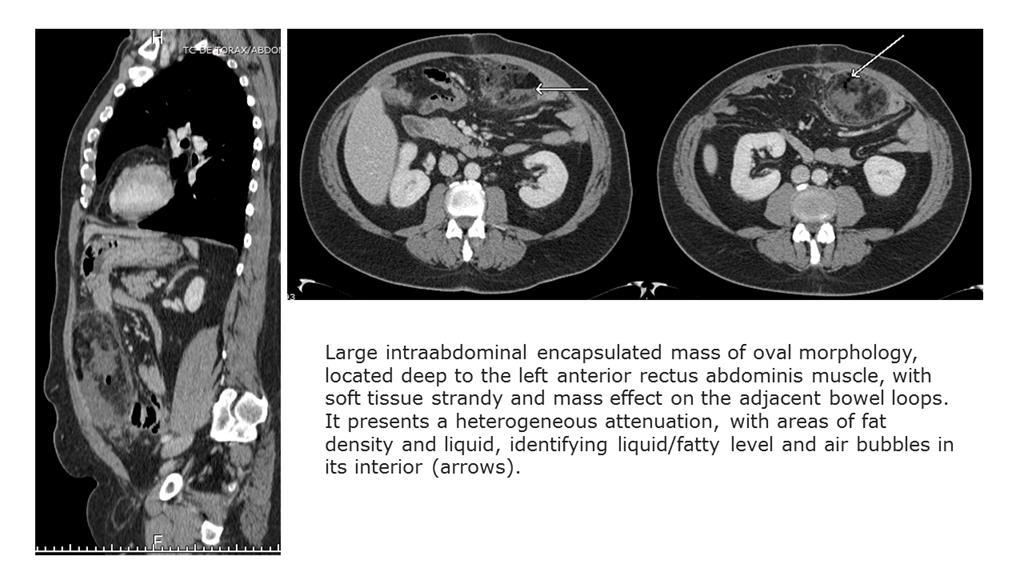
A 60 years old man, who underwent colonic resection four weeks before, come to emergency department with fever, abdominal pain and elevation of acute phase reactants. In the CT we can see a large intraabdominal encapsulated mass (10 x 6 cm) of oval morphology with rim enhancement, located deep to the left anterior rectus abdominis muscle, with soft tissue strandy and mass effect on the adjacent bowel loops. It presents a heterogeneous attenuation, with areas of fat density, liquid and air bubbles in its interior, identifying liquid/fatty level.
Discusión
Epiploic appendagitis and omental infarction are two specific types of fat necrosis that commonly manifest with abdominal pain that mimics acute abdomen, correct identification of these conditions is crucial to avoid unnecessary surgical intervention. Clinically, the differential diagnosis would have to be made with appendicitis, cholecystitis, diverticulitis,…These findings would be related to an omental infarction. Given the surgical history and location, it would be a secondary omental infarction. The liquid/fatty level indicates saponification, and the internal gas indicates infection. It would therefore be an infected secundary omental infarction. At US, omental infarction may appear as a focal area of echogenic fat that corresponds to the site of focal tenderness.With CT the typical differential diagnosis would have to be made with epiplyic appendicitis, which is seen in the CT as a small area of oval morphology and fat attenuation although of greater density than the fat of the normal peritoneum, surrounded by a peripheral ring corresponding to the adjacent inflamed visceral peritoneum, which constitutes the "sign of the ring". Occasionally, a hyperdense focus corresponding to the thrombosed vein or internal hemorrhage may be seen in the center.
Conclusión
Epiploic appendagitis and omental infarction each have a characteristic appearance, but they may mimic other causes of acute abdomen.Omental infarctions usually present with subacute onset of pain in the right lower quadrant, often with a slightly elevated white blood cell count. The omental infarctions can be primary or secondary. Primary omental infarction is often a hemorrhagic infarction resulting from vascular compromise, and its typical location is the right lower quadrant. Secundary omental infarction may occur after atraumatic injury as a result of surgical trauma. Often the site of secundary infarction is near the surgical site. Sometimes the omental infarction can be saponified, appearing a liquid/fatty level, which can favor the superinfection and condition an abscess. It tends to be self-limited and have conservative management, although it may require surgical treatment and may be complicated by abscess.
Bibliografía
- Ramos B, Cuadra A, González M, Pardo S, DoraoM, Gelabert M. Abdomen agudo por necrosis grasa intraabdominal ¿Qué ha de conocer el radiólogo general? SERAM 2014/S-0017 - Kamaya A, Federle M, Desser T. Imaging Manifestations of Abdom