Hospital: HU Virgen de la Victoria.
Nº: C2019-310
Aut@r o Autores: M.D.M. García Gallardo, G.C. Müller Bravo, I. Garcia Trujillo, A.M. Merchán Páez, A.M. Castaño Ramirez, C. Palma González.
Presentación
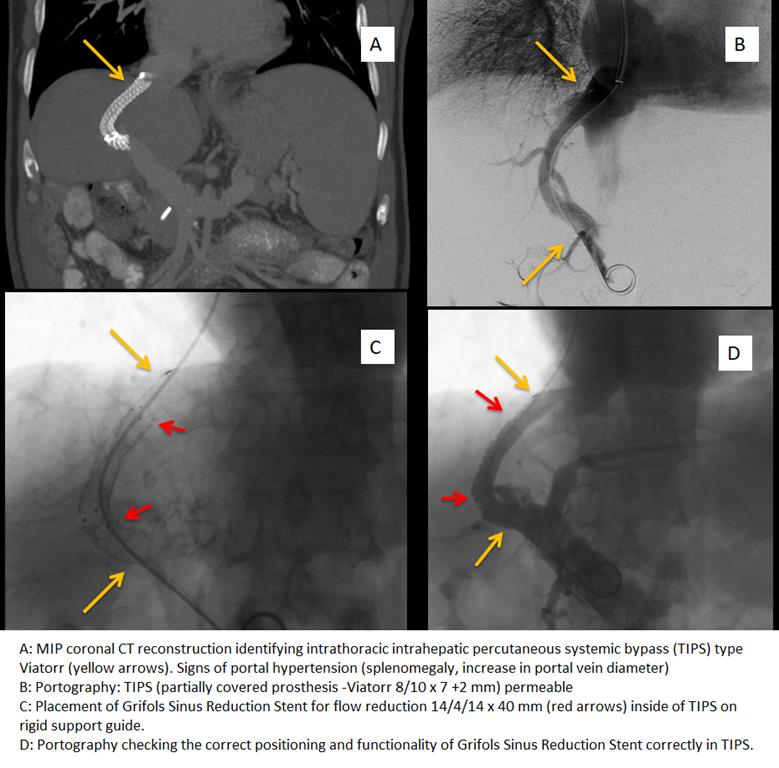
A 53-year-old patient with mixed liver cirrhosis due to HCV and alcohol with portal hypertension (Child-Pugh grade B7). Current treatment: lactulose,Famotidine, Spironolactone,Furosemide,Propranolol. First episode of upper digestive hemorrhage due to esophageal varices, treated with beta-blockers and band protocol. New episode with hemodynamic compromise that required placement of TIPS (partially covered prosthesis -Viatorr 8/10 x 7 +2 mm). In the last months he has presented several income for hepatic encephalopathy (HE) grade III that have remitted with medical treatment. The patient is brought to the emergency department in a comatose state with hyporeflexia and hypotonia. No flapping or asterixis. Manifestations in relation to hepatic encephalopathy (grade IV) after excluding other causes of cerebral involvement analytically and through imaging tests (CT scan of the skull). This EH is resistant to medical treatment, so the endovascular treatment was performed to reduce the size of the TIPS. With right jugular access, the 10F guide wire introducer is inserted and invasive pressures are taken in the portal vein (20mmHg) and in the inferior vein cava (15mmHg). Pressure gradient of approximately 5 mmHg.Then Grifols Sinus Reduction Stent prosthesis for flow reduction 14/4/14 x 40 mm is placed on rigid support guides. Pressure is obtained in a holder of 25 mmHg. Pressure gradient of approximately 10 mmHg.
Discusión
The use of TIPS intrahepatic percutaneous portosystemic shunt in secondary prevention of variceal bleeding and in refractory ascites is supported by highlevel evidence in patients with portal hypertension. However, after performing this technique hepatic encephalopathy (HE) is one of the most frequent complications. The main pathogenic mechanism is the presence in the central nervous system of substances of intestinal origin (mainly ammonium) that escape hepatic clearance. The predictive factors that are associated with the appearance of post-TIPS encephalopathy are the previous history of hepatic encephalopathy, followed by advanced age (> 65 years) and reduction of the portosystemic pressure gradient (GPP)below 5mmHg. The appearance or aggravation of this entity occurs in 30-40% of patients being persistent or recurrent of difficult medical management in 3-6% of cases, which will require more aggressive treatments such as reduction or occlusion of the TIPS caliber and / or liver transplantation
Conclusión
The decrease in the size of TIPS is aimed at reducing the derivation of portal blood flow that escapes hepatic metabolism. Reducing the amount of neurotoxic substances of intestinal origin in the systemic circulation improving or solving the state of encephalopathy in a minimally invasive way.
Bibliografía
- Bureau,J.C.Pagan, G.P.Layrargues,S.Metivier, P.Bellot, P.PerreaultPatencyofstentscove redwith polytetrafluoroethylene in patients treated by transjugular intrahepatic portosystemicshunts: long-term results of a randomized multicentre studyLiver Int,27(2