Hospital: Hospital universitario Virgen de la Victoria.
Nº: C2019-446
Aut@r o Autores: I. Salas Coronado, T. Díaz Antonio, E. Cuartero Martinez.
Presentación
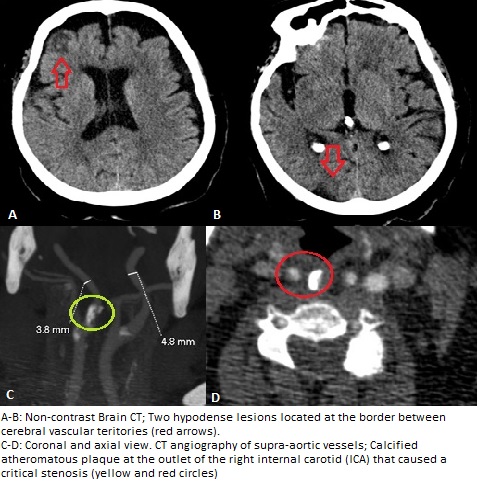
A 72-year-old woman presented to the emergency department with acute onset left hemiparesis (grade 4/5)within the last three hours. She was independent in all activities of daily life, with a personal history of obesity, DM, hypertension, dyslipidemia and depression. A non-contrast Brain CT revealed two hypodense areas of cortical involvment with associatedgyral effacement located in the right frontal and parietal lobes, compatible with evolved acute ischemic stroke. After four days she suffered a worsening of the hemiparesis (grade 1/5) together with dysarthria, left homonymous hemianopia and central facial palsy, coinciding with arterial tension 235/140. The non-contrast CT scan showedtwo new lesions with the same radiological features, also located in the right cerebral hemisphere. The unilaterality of the lesions plus their location at the border between cerebral vascular territories suggest discarding hemodynamic etiology. A CT angiography of the supra-aortic vessels highlighted the presence of a calcified atheromatous plaque at the outlet of the right internal carotid artery (ICA) that caused a critical stenosis with distal hemodynamic repercussion. The Willis polygon was permeable through the communicating branch circulation.?
Discusión
The hemodynamic stroke account for 5-10% of all cerebral infarctions. Episodes of severe systemic hypotension, as cardiac arrest, prolonged syncope or shock, are the typical scenario. It usually occurs in elderly patients with severe stenosis or occlusion of the feeding arteries, in particular the intracranial and extracranial carotid arteries.There are two different border zones infarct: -The cortical/external: between two main cerebral arteries (ACA-MCA or MCA-PCA). -The deep/internal: between MCA cortical branches and perforating lenticulostriate circulation ? Typical imaging appearance in a linear fashion parallel to the lateral ventricles in the centrum semiovale or corona radiata, which sometimes become more confluent and band-like.
Conclusión
Imaging of watershed infarction should aim to determine: - ETIOLOGICAL DIAGNOSIS, in order to prevent the progression of the infarct or early relapse thereof. - VASCULAR STUDY, to detect possible hemodynamically significant stenosing lesions that are accessible to revascularization methods.14.
Bibliografía
- Mangla R, Kolar B,Almast J,Ekholm SE. “Border Zone Infarcts: Pathophysiologic and Imaging Characteristics.”RadioGraphics 2011, 31:1201–1214 - Klijn CJ, Kappelle LJ. “Haemodynamic stroke: clinical features, prognosis, and management”. Lancet Neurol. 2010