Hospital: Hospital Universitario Fundación Alcorcón.
Nº: C2019-269
Aut@r o Autores: C. Machado Orihuela, M. Barxias Martin, A. Cebrian Rivera, D. Dulnik Bucka, C. García-Monco Fernandez, S. Chen Xu.
Presentación
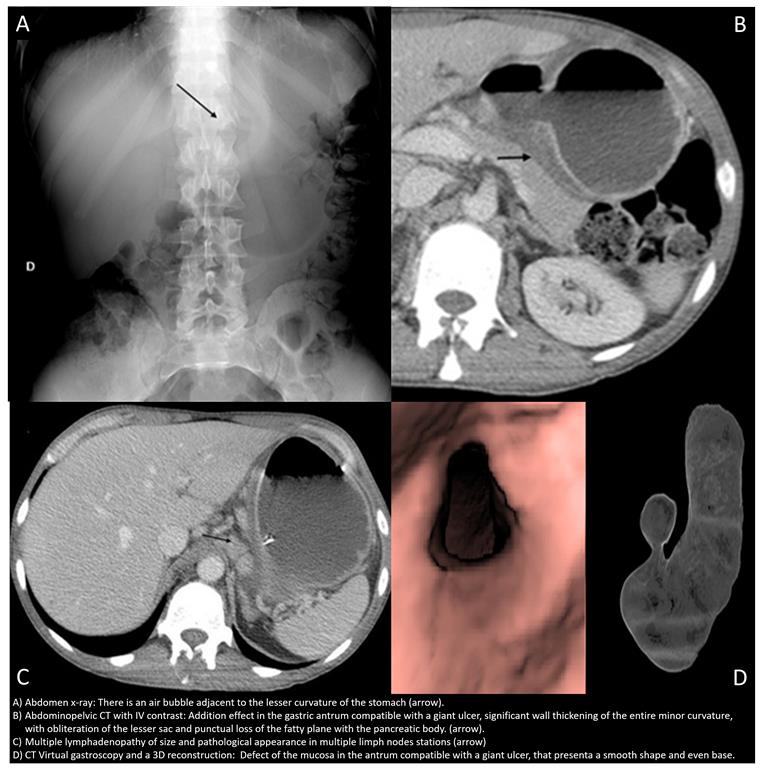
A 40 year old man, smoker, who went to the emergency room for an episode of subacute abdominal pain, important anemization and a 5Kg wieghtloss of three months. An abdominopelvic CT with IV contrast and a CT virtual gastroscopy were performed, identifying a retention stomach with a significant wall thickening of the entire minor curvature, that presented a mamelonated aspect, with obliteration of the lesser sac and punctual loss of the fatty plane with the pancreatic body. In addition, a large contained, regular shape and even base ulcer was seen, without macroscopic perforation findings. Furthermore, multiple locoregional pathologic limph nodes were spotted.
Discusión
These findings suggested that an ulcerated gastric neoplasia had to be rule out. Later on, after two endoscopies and an ecoendoscopy with negative results for malignancy, due to the discordance between the radiologic and endoscopic findings in comparison with de histological findings, a subtotal gastrectomy was performed with the same results. The final diagnosis was a giant benign gastric ulcer. This entity is one of the most frequent pathologies of the stomach, mainly associated with H. pylori infection and NSAISs. It is caused by the rupture of the defensive barrier of the gastric mucosa against the gastric acid that erodes it. The symptoms are varied, from asymptomatic to epigastric pain and weight loss. Often multiple, small and usually benign, it is always important to differentiated it from a malignant ulcer, by examining the morphologic features in CT scan and virtual gastroscopy. Malignant gastric ulcers were identified by irregular, angulated or geographic shapes, bases that were uneven, edges that were irregular or asymmetric, and folds that appeared to be disrupted near the crater edge. Benign gastric ulcers were identified by regular and smooth shapes, bases that were even, edges that were clearly demarcated and regular, and periulcer folds that tapered and converged toward the ulcer.1,2 The treatment consist of proton-pump inhibitors or H2-receptor antagonists, H. pylori treatment if infection, reserving the surgery for recurrent or intratable ulcers, complications and equivocal or suspicious findings on radiologic or endoscopic examinations.
Conclusión
The findings of gastric ulcer in CT sometimes can overlap between both benign and malignant features. Virtual gastroscopy is a recent tool that has proven to be comparableto endoscopy in the differentation between malignant and benign nature, making it a good potential alternative, but requires more studies to investigate the overall efficacy.
Bibliografía
- Chen CY, Kuo YT, Lee CH, Hsieh TJ, Jan CM, Jaw RS, et al. Differentiation between malignant and benign gastric ulcers: CT virtual gastroscopy versus optical gastroendoscopy. Pubmed, Radiology August 2009, Volume 252:number (2) 410-7. - Chen CY, Wu DC