Hospital: Hospital Universitario Puerta de Hierro.
Nº: C2019-209
Aut@r o Autores: M.L. Collado Torres, L. Gómez - Pimpollo García, I. Hernández Delgado, M.D.R. Navarro Torres, M. Alfageme Zubillaga, M.D.P. Reyero Lafuente.
Presentación
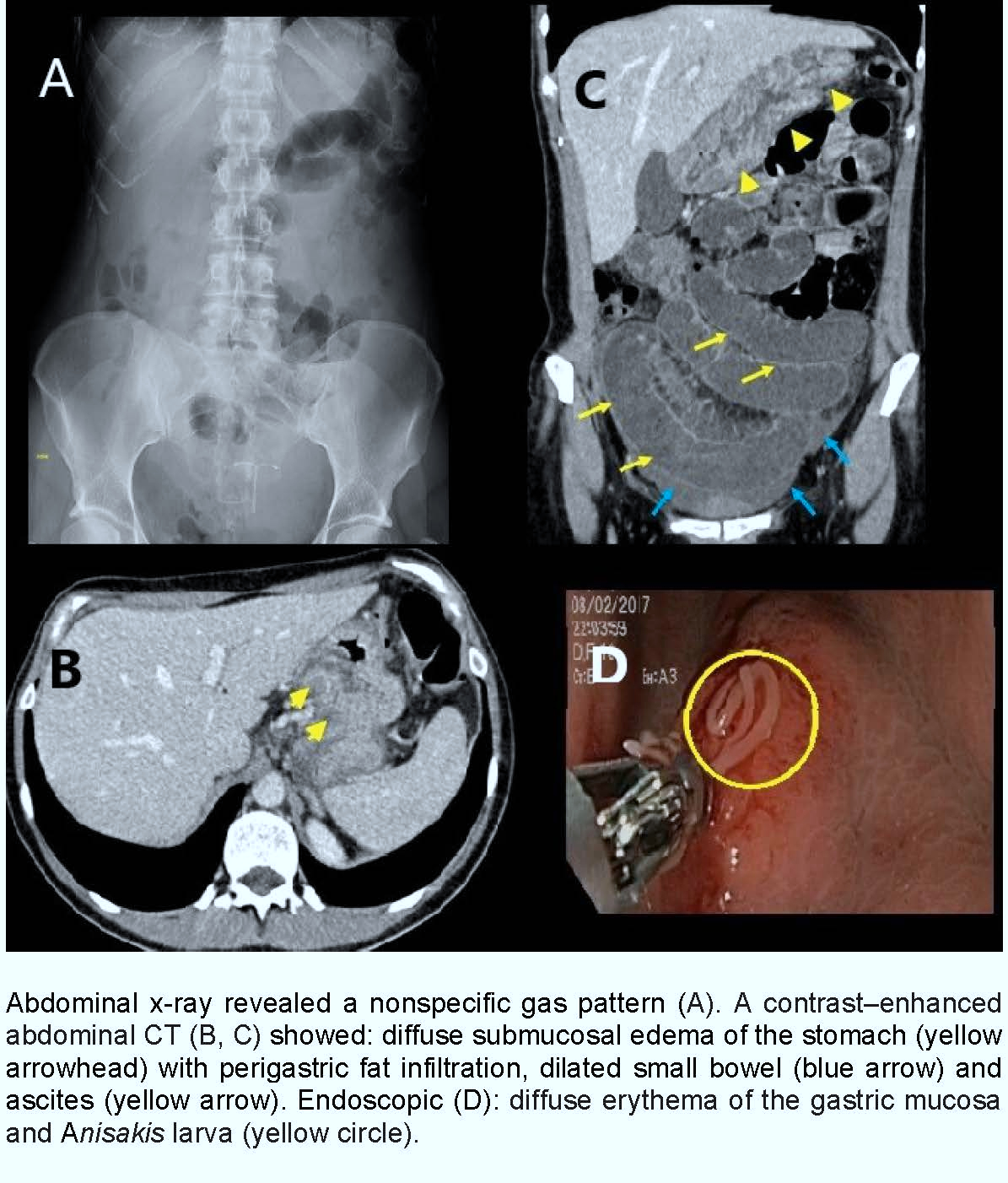
A 41-year-old woman went to the emergency department for acute diffuse abdominal pain and nausea for 24 hours. Non-fever and no other symptoms- signs. Antecedents of interest: IUD and scanty sigmoid diverticulae. Laboratory examinations showed only increased C-reactive protein (24.7 mg/dL) and were otherwise unremarkable. Abdominal x-ray revealed a nonspecific gas pattern (figure). Due to the suspicion of acute diverticulitis was performed a contrast–enhanced abdominal computed tomography (CT), it showed (figure): diffuse submucosal edema of the stomach with perigastric fat infiltration, dilated small bowel (lumen >3cm) and small number of ascites. No signs of acute diverticulitis or other relevant findings.
Discusión
The imaging CT features helped to further elaborate the clinical history of poorly cooked fish consumption. So it was performed an urgent endoscopic showing (figure): diffuse erythema of the gastric mucosa, ulcers and Anisakis larva (at least ten) at the pre pylorus, fundus and body of the stomach (definitive diagnosis), and extraction of Anisakis larva with biopsy forceps (treatment). Anisakiasis is an uncommon zoonotic parasitic infection caused by consumption of raw or undercooked seafood infected with nematodes of genus Anisakis, in our setting the most common source is anchovies in vinegar [1] Clinical manifestations include gastrointestinal forms (from mild pictures with non-specific symptoms to more aggressive forms such as gastroduodenal ulcer, intestinal obstruction or hemorrhagic ascitis) and allergic, mixed and invasive forms in other organs. Gastric involvement is usually more frequent than intestinal infection. Given the non-specific clinical presentation of acute abdomen are often subject to radiologic imaging. Regarding classic and key findings- CT (like this case) are: submucosal edema gastrointestinal, mesenteric or perigastric fat infiltration and ascites. [1,2] Although most are self-limited cases, endoscopic extraction of the larva attached to the gastric mucosa or intestinal resection may be necessary. However, the best treatments are prophylactic measures avoiding intake raw or undercooked fish [1,2]
Conclusión
When CT shows the typical imaging features of gastrointestinal anisakiasis ( submucosal edema with ascites), radiologists may suggest the possibility of clinically undiagnosed anisakiasis. Therefore, abdominal CT is useful for the diagnosis of this infection.
Bibliografía
- Shibata E, Ueda T, Akaike G, Saida Y. CT findings of gastric and intestinal anisakiasis. Abdom Imaging. 2014, 39:257–261. - Takabayashi T, Mochizuki T, Otani N, Nishiyama K, Ishimatsu S. Anisakiasis presenting to the ED: clinical manifestations, time c