Hospital: HCUVA
Nº: C2019-326
Aut@r o Autores: V. Orcajada Zamora, G. Litrán López, A. Navarro Baño, G. De Paco Tudela, A. Castillo García, I. Sánchez-Serrano. HCUVA.
Presentación
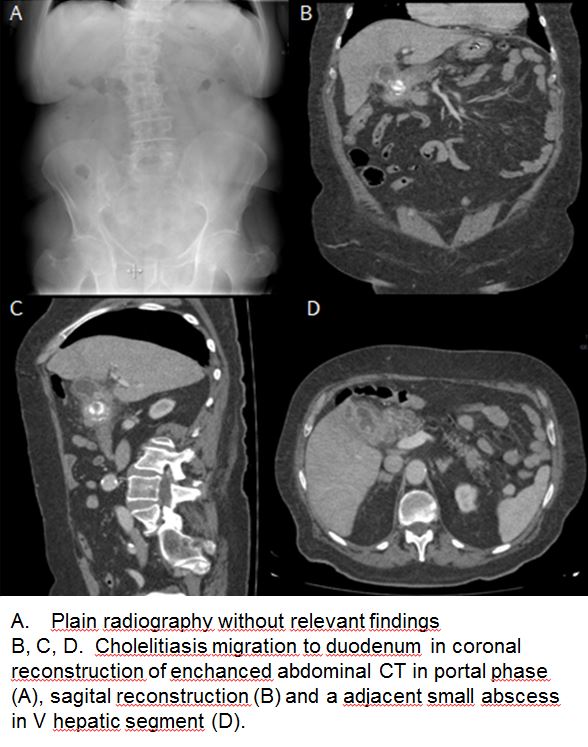
An 81 years old patient with a history of conservatively treated acute cholecystitis, is attended by epigastric abdominal pain and clinical symptoms of intestinal obstruction, with vomits for two days, some of them referred in coffee grounds. On examination, the abdomen was soft and depressible and not painful on palpation. In laboratory tests, only high CRP and neutrophilia without leukocytosis was highlighted. A simple x-ray was performed, where a well positioned nasogastric tube is observed, and scarce air bubbles in the loops and colon, as well as distal air. Slight scoliosis of right convexity. In the absence of relevant findings, an urgent abdominal ultrasound was performed, in which a contracted vesicle with a thickened wall of 4.5 mm was identified, as well as biliary sludge and lithiasis inside it. The findings do not allow us to rule out complicated acute cholecystitis, which is why we decided to expand the study with a CT of the abdomen with contrast. CT showed hyperattenuation of perivesicular fat in relation to perivesicular inflammatory changes, perivesicular edema with parietal thickening and enhancement. A small hypodense collection with peripheral enhancement in the hepatic V segment is also visualized, suggestive of abscess. Ectopic migrated cholelithiasis and impaction in the duodenal bulb was showed This findings are compatible with Bouveret syndrome. No retrograde dilation of the duodenum and stomach is present currently due to nasogastric tube placement.
Discusión
The Bouveret syndrome is a gastric outlet obstruction produced by a gallstone impacted in the distal stomach or proximal duodenum via a gallblader-duodenal fistula. The presenting clinic situation is variable and nonspecific but often includes nausea, vomiting, and epigastric pain. A small minority of patients may present with hematoemesis secondary to duodenum erosions. The rigler triad (bowel obstruction, pneumobilia and ectopic gallstone) is seen only in a minority of patients. US findings may suggest the diagnosis but often present a confusing imaging. The TC increasingly used in emergency department reveal this inusual condition more frequently and next to endoscopic retrograde Cholangiopancreatography are likely the most sensitive modalities for diagnosis
Conclusión
Radiologists should become familiar with the imaging appearance of this condition, which causes significant morbidity and mortality.
Bibliografía
- Mallvaux P, Degolla R, De Saint-Hubert M, Farchakh E, Hauters P. Laparoscopic treatment of gastric outlet obstruction caused by gallstone (Bouveret’s syndrome). Surg Endosc 2002,16:1108–1109. - Singh AK, Shirkhoda A, Lal N et-al. Bouveret's syndrome: