Hospital: HUV Macarena.
Nº: C2019-627
Aut@r o Autores: A. Rivera Dominguez, D. De Araujo Martins Romeo, T. Ruíz Garcia, A. García De La Oliva.
Presentación
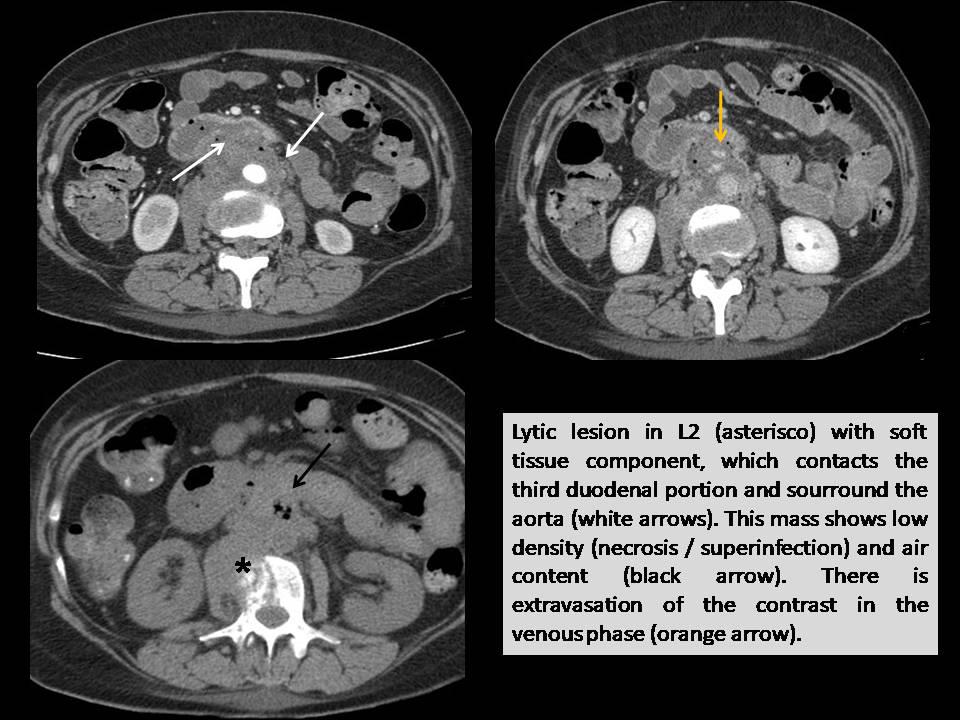
A 49-year-old woman with history of cervix carcinoma and intense back pain for several months consulted with digestive hemorrhage, intense epigastralgia and lumbar pain. During hospital admission an upper gastrointestinal endoscopy (UGE) revealed no bleeding point. Despite blood cells transfusion, she progressed with anemization and hemodynamic instability. An angio- CT revealed a lytic lesion in L2 with soft tissue component, which contacts the third duodenal portion and the aorta, shows air component inside and extravasation of contrast in the venous phase. It is diagnosed with aortoenteric fistula (AEF). The aortography confirmed extravasation of contrast from the posterolateral aspect of the infrarenal aorta to the intestinal lumen and retroperitoneum. The patient was managed first with aorta stenting, and later with surgery to resect the 3rd and 4th duodenal portion (AP: Ca infiltration of squamous cells), and L2 laminectomy with interlaminar stabilization. Unfortunately, the patient dies three months later.
Discusión
AEF is a communication between the aorta and the gastrointestinal tract. They are 2 types of AEF: primary (PAEF), or secondary (SAEF) according to whether or not they are associated with a history of graft repair (1,2). PFAE are mainly due to aortic aneurysms (AA), mostly arteriosclerotic. Other infrequent causes are: irradiation, metastasis, pancreatic carcinoma, ulcers, biliary lithiasis, diverticulitis, appendicitis and cystic necrosis of the aorta media (1,2). Although it can affect any part of the gastrointestinal tract, the third and fourth portions of the duodenum are affected in 82% of cases (1). The main symptom is upper gastrointestinal bleeding, that characteristic presents with a minor "heraldic hemorrhage" in which a self-limiting bleeding precedes a massive hemorrhage. Other signs and symptoms include: abdominal pain, pulsatile abdominal mass, back pain, fever and sepsis (1). Although an UGE is the method of choice to evaluate digestive bleeding, a negative study doesn´t rule out an AEF. Angio-CT has a sensitivity of 40-90% and a specificity of 33-100%. The findings that can be found are: extravasation of contrast from the aorta to the intestine, gas adjacent or inside the aorta, loss of the periaortic fatty plane, retroperitoneal or intestinal wall hematoma. Angiography is of limited use in diagnosis, especially if the rate of blood loss is slow (1). Mortality from untreated ADF is almost 100%. Standard treatment for AEP is surgerywith repair of duodenal fistula and AA (2).
Conclusión
PAEF should be considered the cause of UGIB in patients with AA unless the origin of the bleeding has been unequivocally identified.
Bibliografía
- Lemos D, Raffetto J, Moore C, Menzoian J. Primary aortoduodenal fistula: a case report and review of the literature. J Vasc Surg. 2003, 37:686-9. - Alzobydi AH, Guraya SS. Primary aortoduodenal fistula: a case report. World J Gastroenterol. 2013, 19: