Hospital: Hospital Vall d'Hebron.
Nº: C2019-501
Aut@r o Autores: A. Antón Jiménez, D. Moreno Martínez, E. Castellà Fierro, E. Moraru, A. Roque Pérez, H. Cuéllar Calabria.
Presentación
A 82 year-old male patient with a history of hypertension and arthrosis, presented with back pain. An ambulatory spinal MRI showed lumbar degenerative disc disease without discal hernia and incidentally, an aneurysmatic dilatation of the abdominal aorta with a maximum diameter of 5 cm. One week later the patient refered an acute onset of abdominal pain with dorsal irradiation together with pain and palsy of the lower extremities and hemodynamical unstability.?
Discusión
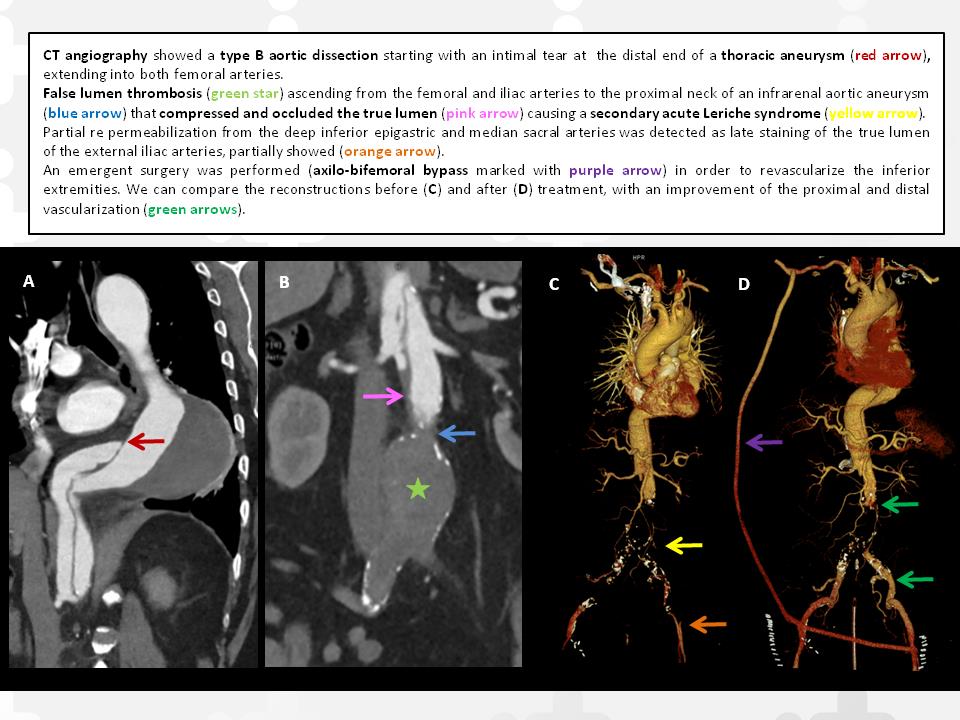
A CT angiography was performed in the ER department. It showed: - An aneurysm of the distal descending thoracic aorta (diameter of 8,5 cm) with a large mural thrombus. - A type B aortic dissection starting as an intimal tear at the distal end of the thoracic aneurysm and extending into both femoral arteries. - False lumen thrombosis ascending from the femoral and iliac arteries to the proximal neck of an infrarenal aortic aneurysm (diameter of 6 cm). - The celiac trunk, superior mesenteric and renal arteries originated in the patent suprarenal false lumen.- The thrombosed false lumen of the infrarenal aneurysm compressed and occluded the true lumen (causing a secondary acute Leriche syndrome). - Partial re permeabilization from the deep inferior epigastric and median sacral arteries was detected as late staining of the true lumen of the external iliac arteries.The main diagnosis was acute Leriche syndrome secondary to thrombosis of the false lumen in a type B aortic dissection. Reviewing the literature, we did not find any similar case. An emergent surgery was performed in order to revascularize the inferior extremities, with an axilo-bifemoral bypass. The patient is now asymptomatic.Although the main cause of Leriche syndrome is atherosclerosis, other occlusive causes should be taken into account, especially when there is an acute onset, as in this case. Ischemic of the visceral circulation is the main prognostic factor in acute type B dissection. In this case, the celiac trunk , mesenteric and renal arteries were patent, without signs or symptoms of abdominal ischemia, and a successful revascularization was possible. Extension of a type B dissection into the iliac or femoral arteries has implications for management, especially when percutaneous intervention is being considered. In our case this option was not possible since there was a thrombosis of the false lumen.?
Conclusión
Aortic dissection is the most common acute emergency condition of the aorta and often has a fatal outcome. Imaging techniques are essential for a correct emergent approach. 16.
Bibliografía
- McMahon MA and Squirrell CA. Multidetector CT of Aortic Dissection: A Pictorial Review. Radiographics RSNA 2010, 30: 445-460. - Chong BK and Kim JB. Successful Surgical Treatment for Thoracoabdominal Aortic Aneurysm with Leriche Syndrome. Korean J Thora