Hospital: Hospital Morales Meseguer, Hospital Santa Lucía.
Nº: C2019-560
Aut@r o Autores: B. Márquez Argente Del Castillo, J. Plasencia Martínez, M. Plasencia Martínez, M. Gayán Belmonte, A. García Chiclano, I. García Tuells.
Presentación
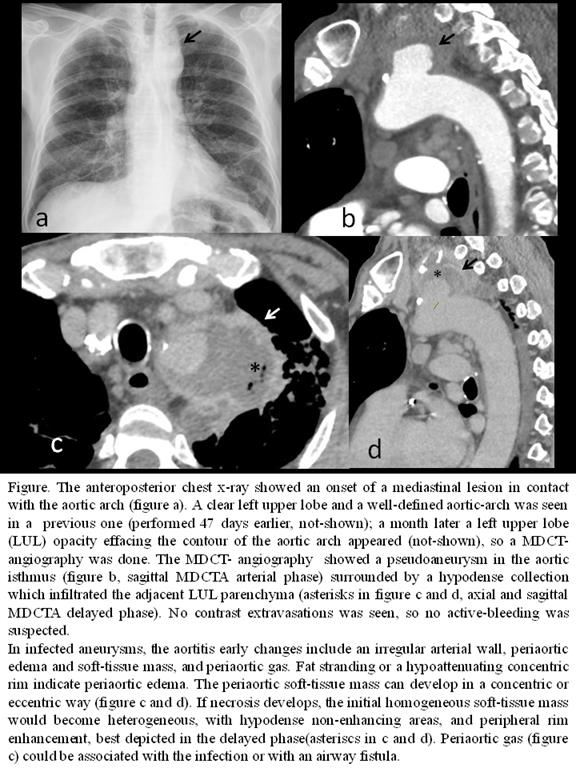
A 79 year-old male presented to the emergency department with significant haemoptysis. During the last months, he suffered from perforated duodenal ulcer and appendicitis with pylephlebitis, with surgical treatment only for the first. Imaging findings: An anteroposterior chest x-ray performed at the emergency department showed a new onset of a mediastinal lesion in contact with the aortic arch (figure a), not visible in recent studies and with left upper lobe (LUL) extension later (not shown). As the patient had haemoptysis, an aortic MDCT-angiography was performed. MDCT in arterial phase (figure b) demonstrated a pseudoaneurysm in the aortic isthmus surrounded by a collection with air bubbles, which infiltrated the adjacent LUL parenchyma. Immediately, a delayed phase was obtained (figures c-d) which highlighted enhancement of the ill-defined collection wall. No active-bleeding was revealed. A septicaemia by Prevotella spp and Bacteroides fragilis was detected. The patient was treated with endoluminal stent-graft placement and antibiotics. He evolved favourably.
Discusión
Although parenchymal or airway infection are the cause of 70% of haemoptysis [1], a serious vascular disease, not previously suspected and revealed by MDCT-angiography, was the cause in our patient: An infected aortic aneurysm or “mycotic aneurysm”. It is defined as an infectious break in the wall of an artery with formation of a saccular outpouching that is contiguous with the arterial lumen (pseudoaneurysm) [2]. They can develop from a normal aorta or from a pre-existing aneurysm due to infectious microemboli in the vasa vasorum during bacteraemia (most common), contiguous involvement from an adjacent focus or direct inoculation. Differently from atherosclerotic aneurysm, infected aneurysms commonly occur in the thoracic or suprarenal abdominal aorta [3]. To determine the cause and treatment of a lifethereating haemoptysis, an urgent MDCT angiography should be performed. To know the radiological manifestations (see figure) and to check with the personal antecedents is crucial to diagnose this entity. Aortic infected aneurysms have traditionally been treated by prompt open surgery in combination with antibiotics, but endovascular techniques are becoming a strong alternative [2], as in our case.
Conclusión
Infected aortic aneurysms are uncommon but lifethreatening condition. In the thoracic aorta they can manifest with haemoptysis. Timely diagnosis with MDCT and early intervention are crucial to optimise patient outcome.
Bibliografía
- Bidwell JL, Pachner RW. Hemoptysis: diagnosis and management. Am Fam Physician. 2005,72: 1253-60. - Lee WK, Mossop PJ, Little AF, Fitt GJ, Vrazas JI, Hoang JK, Hennessy OF. Infected (mycotic) aneurysms: spectrum of imaging appearances and management.