Hospital: HULP
Nº: C2019-507
Aut@r o Autores: E. Lanz Santos, Á. Díez Tascón, M. Caicoya Boto, A.J. Barrios López, F. García Marínez, M. Martí De Gracia.
Presentación
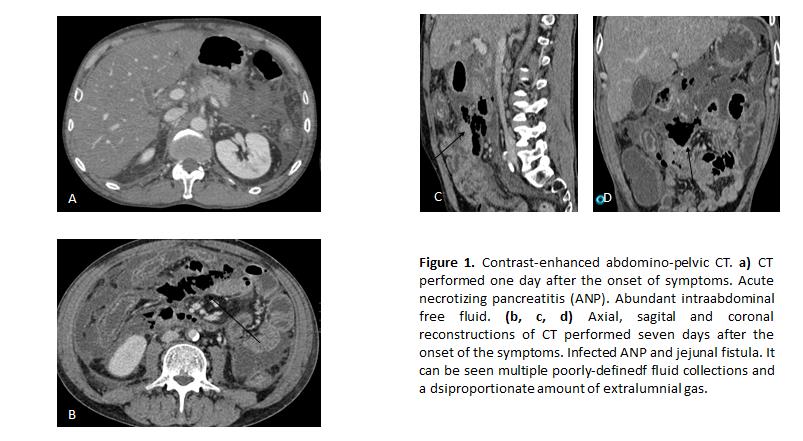
A 54-year-old male attended the emergency services referring intense epigastric pain, nausea and vomits. Laboratory studies revealed high serum levels of amylase. He was diagnosed of acute pancreatitis and admitted for conservative management. During the next seven days the patient developed fever and evident clinical deterioration, being transferred to the intensive care unit. A contrast enhanced-CT was performed. The CT showed acute combined necrotic pancreatitis. It could be observed diminished enhancement and enlargement of pancreatic distal body and tail, as well as multiple acute necrotic collections in peripancreatic, subhepatic and parietocolic spaces and mesenteric root, which presented poorly defined walls and nonliquefied components. It was also identified a great amount of gas within the collections and peritoneal enhancement. Infection of the collections was suspected. The patient underwent emergency laparotomy which demonstrated purulent peritonitis, multiple abscesses and a 0,5 cm perforation in proximal jejunum (which could not be identified on CT).
Discusión
Necrotizing pancreatitis (ANP) accounts for 5%–10% of cases of acute pancreatitis. The necrosis may involve either the pancreatic parenchyma and/or the peripancreatic tissues. There have been described three types of ANP: pancreatic only (nonenhancing pancreas), peripancreatic only (nonenhancing heterogeneous peripancreatic collections) and combined. Infection occurs as a complication in 20% of patients with necrotizing pancreatitis, commonly 2-4 weeks after presentation. At imaging, the presence of gas within a collection suggests infection (although it is only found in a minority of confirmed cases), but it can be also the result of a gastrointestinal fistula. Wall enhancement is not a reliable indicator of infection. Fistulas are defined as pathological communications that connect any portion of the gastrointestinal tract with the necrotic cavity, the peritoneal space, the retroperitoneal areas, or another internal organ. They are a rare complication of acute necrotizing pancreatitis which result from the erosion of the bowel wall by the necrotic collection, most commonly in the colon and the duodenum. Conventional contrast enhanced CT has a low sensitivity in the detection of this pathology, having been proposed the usage of rectal and oral contrasts to improve its outcome.
Conclusión
Acute necrotizing pancreatitis is a severe form of acute pancreatitis characterized by necrosis in and/or around the pancreas. The presence of gas within the necrotizing collections usually suggests infection, although in rare cases it can be the result of the formation of a gastrointestinal fistula.
Bibliografía
- Revised Atlanta Classification for Acute Pancreatitis: A Pictorial Essay. Bryan R. Foster et al. RadioGraphics 2016, 36:675–87. - Necrotizing Pancreatitis: Diagnosis, Imaging, and Intervention. Jeffrey Y. Shyu. RadioGraphics 2014, 34:1218–39. - Gastr