Hospital: General University Hospital Morales Meseguer.
Nº: C2019-134
Aut@r o Autores: I. Vicente Zapata, A. Blanco Barrio, B. Márquez Argente Del Castillo.
Presentación
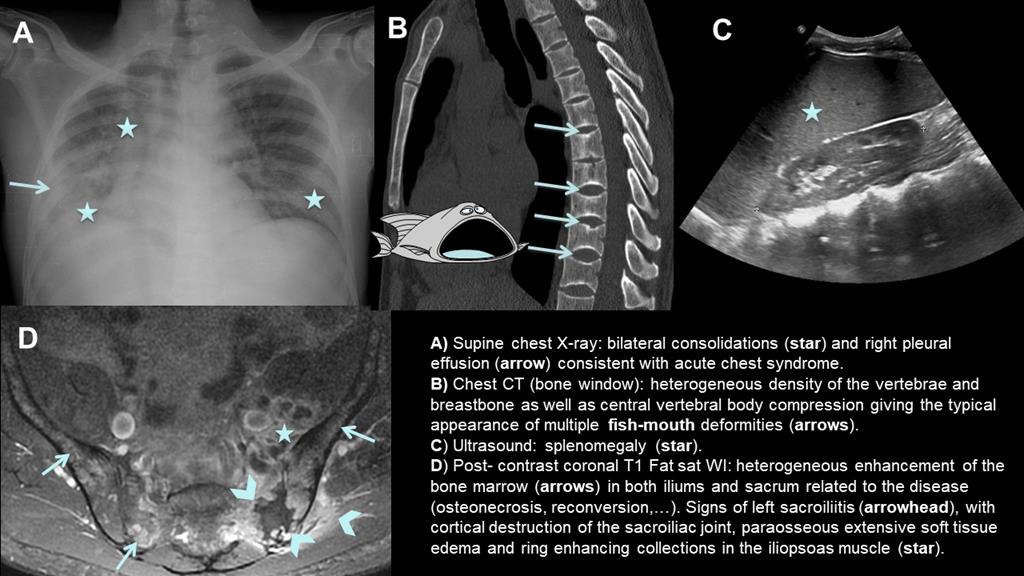
A 30-year-old man from Ivory Coast presenting with high temperature, respiratory failure, abdominal and back pain and intense asthenia. Blood analysis showed sepsis signs and anemia and different imaging modalities were performed: chest X-ray showed bronchopneumonia and right pleural effusion consistent with acute chest syndrome, abdominal ultrasound with splenomegaly thought to be sequestration syndrome since the patient required blood transfusion, chest CT with bone window where fish-mouth vertebral deformities were seen and sacrum MRI showed bone marrow signal alteration with bilateral sacroiliitis plus left joint collections extending to the iliopsoas muscle (Fig. 1). In the meantime, the blood culture showed salmonella and a blood frotis and hemoglobin electrophoresis were performed showing sickle cells and hemoglobin S which confirmed the diagnosis.
Discusión
Sickle cell anemia (SCA) is an autosomal recessive hereditary disorder, hemolytic anemia characterized by defective hemoglobin (Hb) synthesis with production of an abnormal form, known as sickle hemoglobin (Hb S), which is rigid and sticky (sickle shaped) and produce thrombosis with multisystem repeated vessel occlusion and ischemia [1-3]. The highest incidence occurs in sub-Saharan Africa regions where it confers a human genetic resistance to malaria [1, 2]. The first presentation is commonly acute, with an abdominal painful vaso-occlusive crisis often in the setting of sepsis [2]. Complications of SCA are wide and affect different system: - Musculoesketal: this is the most frequent affected [1-3], either by excessive intramedullary and extramedullary hematopoiesis, which result in expansion of the medullary spaces, osteonecrosis (mostly ephyseal) or increased susceptibility of septic arthritis/osteomyelitis, due to repeat bone infarcts which result in osteopenia and central vertebral body compression giving the typical appearance of multiple fish-mouth or H-shaped vertebrae. - Abdominal:the most commonly involved organ is the spleen [3]. Renal, liver or spleen infarctions are often seen, with a subsequent asplenia in final phases. Mesenteric vaso-occlusive crisis are also present. An unusual but life-threatening complication of SCA is sequestration syndrome, a rapid pooling of the blood within solid organs (usually the spleen), causing acute organomegaly and vascular collapse. - Pulmonary: it can be acute or chronic. Acute chest syndrome (ACS) is another life-threatening complication [2, 3]. ACS is defined as a new consolidation and/or pleural effusion on chest radiograph, associated with respiratory symptoms. - Cerebrovascular accidents and cardiovascular complications.
Conclusión
Presentation of SCA may involve any system of the body, thus different types of imaging techniques are needed for a correct recognition of radiological features that lead to a precise diagnosis.
Bibliografía
- Ejindu VC, Hine AL, Mashayekhi M, Shorvon PJ, Misra RR. Muskuloeskeletal Manifestations of Sickle Cell Disease. Radiographics, 2007, 27: 1005–22. - Lonergan GJ, Cline DB, Abbondanzo, SL. Sickle Cell Anemia. Radiographics, 2001, 21: 971–994 - Agha M, E